We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Hip dislocation
From WikEM
Contents
Background
- Orthopedic emergency; reduction of native hips should occur within 6hr due to high risk of avascular necrosis
- High-energy trauma is primary mechanism
Types
- Posterior
- 90% of hip dislocations
- Acetabular fractures may result as well
- Anterior
- 10% of hip dislocations[1]
- Can be superior (pelvic) or inferior (obturator)
- Neurovascular compromise is unusual
Clinical Features
- Posterior Dislocation
- Extremity is shortened, internally rotated, adducted
- Often Knee-to-Dashboard
- Assess neurovascular exam
- Sciatic nerve is most common compromised
- Anterior Dislocation
- Extremity is extended (superior) or flexed (inferior), externally rotated, abducted[2]
- Similar to hip fracture
Differential Diagnosis
Hip pain
- Femur fracture
- Hip dislocation
- Hip bursitis
- Psoas abscess
- Piriformis syndrome
- Meralgia paresthetica
- Septic Arthritis (Hip)
- Obturator nerve entrapment
- Pelvic fractures
- Avascular necrosis of hip
Evaluation


- Hip AP and lateral views
- Posterior Dislocation: AP view femoral head posterior and superior to acetabulum
- Anterior Dislocation: AP view shows femoral head in obturator foramen (inferior to acetabulum)
- If associated femoral neck fracture, will likely need orthopedics
- Consider Judet views
- Consider knee xray
- Consider CT to evaluate acetabulum for subtle fractures (esp for posterior dislocation)
Management
- Reduction recommended within 6 hours to prevent avascular necrosis of the femoral head[3]
- Procedural sedation
Posterior
- Allis Maneuver: supine patient on table: deeper sedation (propofol helps with tissue relaxation); firm distal traction at flexed knee to pull head back into acetabulum; assistant stabilizes pelvis by pushing on ASISs
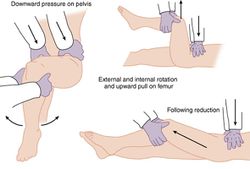
Anterior
- Reduction: traction, internal rotation, and then external rotation once the femoral hip clears the acetabular rim
Captain Morgan Hip Reduction[4]
- See figure here
- See video here
- Provider's knee behind supine patients flexed knee with anterior force lifting (via provider plantar flexing foot) and rotation as needed
- Successful in patients with prosthetic hips as well
- Poses less risk of knee injury since most force is applied by lifting leg rather than applying leverage at knee
- Less risk to provider who does not have to stand on top of gurney, and requires only one provider
{kind=link}
Disposition
- If reduced, outpatient with ortho follow up
Post Reduction Care
- Maintain dislocation precautions:
- Do not bend the operated hip past 90 degrees (use knee immobilizer as needed)
- Do not cross the midline of the body with operated leg (use hip abduction pillow)
- Do not rotate the operated leg inward
- In bed, toes and knee cap should point toward ceiling
- Toe touch weight bearing
Complications
- Post-traumatic arthritis
- 20% in simple dislocations
- high in complex dislocations
- Femoral head osteonecrosis
- 5-40% incidence
- Delay in treatment >6 hours can lead to avascular necrosis of the femoral head => osteonecrosis
- Sciatic nerve injury
- 8-20% incidence
- associated with longer time to reduction
- Recurrent dislocations: <2%
Video
References
- ↑ Holt GE and McCarty EC. Anterior hip dislocation with an associated vascular injury requiring amputation. J Trauma. 2003; 55(1):135-138.
- ↑ Alonso JE, et al. A review of the treatment of hip dislocations associated with acetabular fractures. Clin Orthop Relat Res. 2000; 377(8):32-43.
- ↑ Jaskulka RA, et al. Dislocation and fracture-dislocation of the hip. J Bone Joint Surg Br. 1991; 73(3):465-469.
- ↑ Hendey GW and Avila AA. The Captain Morgan Technique for the Reduction of the Dislocated Hip. Annals of Emergency Medicine, Volume 60, Issue 1, July 2012, Pages 135-136.