We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Hypertrophic cardiomyopathy
From WikEM
Contents
Background
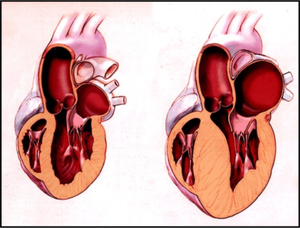
- Genetically-linked (AD) hypertrophy of cardiac muscle - can but does not always cause outflow obstruction
- Up to 30% of patients will have no family history[1]
- Average age of diagnosis between 30-40 years of age
- Diastolic heart failure
- Abnormal LV function due to decreased compliance
- Historically, obstructive forms known as:
- Idiopathic hypertrophic subaortic stenosis (IHSS)
- Asymmetric septal hypertrophy (ASH)
- Hypertrophic obstructive cardiomyopathy (HOCM)
- Yamaguchi syndrome, an atypical HCOM, in which only 1% are non-Japanese
Clinical Features
- Syncope, chest pain, dyspnea
- Symptoms made worse by exertion
- Increasing ventricular contractility further narrows outflow as volume is lost
- Systolic murmur increases with valsalva
- Decreased blood return to heart
- Systolic murmur decreases with squat/fist clench
- Increased peripheral resistance increases aorta and reduces obstruction
Differential Diagnosis
Cardiomyopathy
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
- Restrictive cardiomyopathy
- Peripartum cardiomyopathy
- Takotsubo cardiomyopathy
- Arrhythmogenic right ventricular dysplasia
Chest pain
Critical
- Acute Coronary Syndromes
- Aortic Dissection
- Cardiac Tamponade
- Pulmonary Embolism
- Tension Pneumothorax
- Boerhhaave's Syndrome
- Coronary Artery Dissection
Emergent
- Pericarditis
- Myocarditis
- Pneumothorax
- Mediastinitis
- Cholecystitis
- Pancreatitis
- Cocaine-associated chest pain
Nonemergent
- Stable angina
- Asthma exacerbation
- Valvular Heart Disease
- Aortic Stenosis
- Mitral valve prolapse
- Hypertrophic cardiomyopathy
- Pneumonia
- Pleuritis
- Tumor
- Pneumomediastinum
- Esophageal Spasm
- Gastroesophageal Reflux Disease (GERD)
- Peptic Ulcer Disease
- Biliary Colic
- Muscle sprain
- Rib Fracture
- Arthritis
- Chostochondirits
- Spinal Root Compression
- Thoracic outlet syndrome
- Herpes Zoster / Postherpetic Neuralgia
- Psychologic / Somatic Chest Pain
- Hyperventilation
- Panic attack
Evaluation
- Symptoms: Syncope or sudden death most common
- Also exertional dyspnea, chest pain, syncope, dizziness, palpitations, or CHF
- Systolic murmur that increases with maneuvers that decrease preload (e.g. valsalva, transitioning from squatting to standing, etc.).
- ECG
- Nonspecific/normal.
- Or, high voltage/LVH, deep narrow Q waves in 1, avL, V5, V6 = "daggers of death"

Work-Up
- ECG abnormalities in ~90%, but mostly nonspecific
- High voltage ECG (which may produce abnormal T-waves)
- LVH
- Left atrial enlargement
- Tall R-wave in V1, mimicking posterior MI
- "Needle-like" Q waves, especially in lateral leads, mimicking infarction Q waves
- CXR may be normal as LV is non-dilated
- Echo[2]
- Unexplained wall thickness > 15 mm in any myocardial segment
- Septal/posterior wall thickness ratio:
- >1.3 in normotensive pts
- >1.5 in hypertensive pts
- Systolic anterior motion by M mode in PSL window, worsened by Valsalva
- Mitral regurgitation
- EF may be preserved until acute decompensation
- Formal echo should include tissue Doppler imaging
Management
- Avoid exertion
- ICD +/- pacer for ventricular arrhythmias
- Definitive treatment is myomectomy
Decompensated
- Consider primary insult, which usually is preload issue (fluid depletion, bleed, etc.)
- If decompensated presents as hypotensive CHF
- Preserve preload
- Careful hydration
- Avoid high airway pressure if intubate
- Limit tachycardia
- Beta blockers
- Avoid vasodilators (no nitrates)
- Maintain sinus rythm (i.e. cardiovert A. fib)
- Increase afterload (hypotensive only)
- Phenylephrine, max dose range depending on source
- Start at 100 mcg/min (~1.5 mcg/kg/min for average adult)
- Range usually 0.5 - 6.0 mcg/kg/min, with efficacy minimal beyond 6 mcg/kg/min)[3]
- Max phenylephrine infusion before other pressors
- Fix acid-base disorder as acidosis may prevent pressor efficacy
- Consider maxing vasopressin next
- Pressor effects more preserved in hypoxia and acidosis[4]
- Preferred over pressors with beta agonism
- Push dose pressor while waiting for IV drip:
- Place 1mL of 10mg/mL phenylephrine in 100mL NS
- Final concentration 100mcg/mL
- Use 1-2mL q2-5min (100-200mcg) in 10mL syringe
- Onset 1min; duration 20min
- Phenylephrine, max dose range depending on source
- Preserve preload
Pharmacologic Management
- Per Amer Coll of Cardiology 2011 recommendations[5]
- Class I
- beta-blockers for angina or dyspnea in adults in HCM regardless of obstructive physiology - use with caution in sinus brady or conduction abnormality
- Titrate BB dose to symptoms, may increase BB dose to resting HR to 60 bpm
- PO verapamil titrated up to 480mg/d if patient unresponsive or cannot tolerate beta-blockers - caution in advanced HF, hypotension, sinus brady, high LVOT gradients
- IV phenylephrine for acute hypotension unresponsive to fluids
- Class IIa
- Reasonable to add disopyramide with BB or verapamil if unresponsive to BB or CCB alone in obstructive HCM
- Reasonable to add oral diuretics in nonobstructive HCM when symptoms persist despite BB or CCB
- Class III (harm)
- Avoid nifedipine and other dihydropyridine CCB
- Avoid digitalis
- Avoid disopyramide alone with out BB or CCB
- Avoid positive inotropic vasopressors (dopamine, dobutamine, norepinephrine, epi)
Disposition
- Admit for echo and cardiology evaluation
- If unable to admit, home on beta blocker, instructions for no exertion, follow up echo and cardiology outpt
See Also
References
- ↑ Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE, Towbin JA, Udelson JE, Yancy CW. 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy: Executive Summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force of Practice.
- ↑ Mitevksa IP. Focus on echocardiography in hypertrophic cardiomyopathy - fourth in series. ESC Council for Cardiology Practice. Vol.13,N°20 - 14 Apr 2015.
- ↑ Global RPH in reference to Micromedex. 12/2014. http://www.globalrph.com/phenylephrine_dilution.htm
- ↑ Overgaard CB and Dzavik V. Contemporary Reviews in Cardiovascular Medicine: Inotropes and Vasopressors - Review of Physiology and Clinical Use in Cardiovascular Disease. Circulation. 2008; 118: 1047-1056.
- ↑ American College of Cardiology. 2011. http://content.onlinejacc.org/article.aspx?articleid=1147838