We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Arrhythmogenic right ventricular dysplasia
From WikEM
Contents
Background
- ARVD is a significant contributor to sudden cardiac death in young patients
- Second most common cause of sudden cardiac death in young adults and athletes after hypertrophic obstructive cardiomyopathy (HOCM)
- More common in males and those of Mediterranean descent
- M:F = 3:1
- 1:1000-10,000 in the US
- Fibro-fatty replacement of myocardium
Clinical Features
- Palpitations (27%)
- Syncope (26%)
- Ventricular dysrhythmia/cardiac arrest (23%)
- Family history of unexplained syncope or sudden death
- Dysrhythmias refractory to anti-dysrhythmic meds
- Asymptomatic (40%)
- Usually these patients are identified through genetic testing of an affected or symptomatic family member
- Right ventricular failure (6%)
- Dyspnea
- Atypical chest pain (6%)
Differential Diagnosis
Cardiomyopathy
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
- Restrictive cardiomyopathy
- Peripartum cardiomyopathy
- Takotsubo cardiomyopathy
- Arrhythmogenic right ventricular dysplasia
Syncope Causes
- Cardiovascular-mediated syncope
- Dysrhythmias:
- WPW (pre-excitation)
- Long QT Syndrome
- Brugada Syndrome
- 2nd/3rd AV Block
- Afib/aflutter
- Vtach/torsades
- Sick sinus syndrome
- Arrhythmogenic right ventricular dysplasia
- Short QT syndrome
- Cardiovascular disease
- Valvular Disease (AS, MS, tricuspid stenosis)
- Aortic Dissection
- Myocardial Infarction
- CHF
- Hypertrophic Cardiomyopathy
- PE
- Pericardial Tamponade
- Myxoma
- Pulmonary Hypertension
- Pacemaker malfunction
- Dysrhythmias:
- Neurally mediated syncope
- Vasovagal:
- Fear, pain, emotion, valsalva, breath-holding spell
- Situational (associated with):
- Coughing, micturition, defecation, vomiting
- Carotid sinus stimulation
- Vasovagal:
- Orthostatic hypotension-mediated syncope:
- Volume depletion:
- Autonomic Dysreflexia
- Autonomic failure due to meds
- Other serious causes
- Stroke
- SAH
- TIA
- Vertebrobasilar Insufficiency
- Subclavian steal
- Heat syncope
- Hypoglycemia
T Wave Inversions
- Normal in pediatrics
- Myocardial infarct (NSTEMI)
- Myocardial ischemia (Wellen's) - T waves go up, then down
- Hypokalemia - T waves go down, then up (or camel humped, one upright TW and upright U-wave in severe hypokalemia)
- Hyperkalemia
- Pulmonary embolism (RV strain)
- Pulmonary hypertension, acute or chronic
- Pulmonary disease - hyperventilation, pneumothorax, pneumonia
- LVH with strain pattern
- RVH
- Bundle branch block (both left and right)
- WPW
- Pericarditis (stage 3)
- CNS T waves (diffuse, deep)
- Arrhythmogenic right ventricular dysplasia (may also have epsilon wave)
- HOCM
- Paced rhythm
- Elevated intracranial pressure
Evaluation
ECG
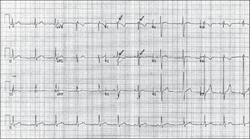
- Epsilon wave (30-50%)
- V1-V3 TWI (especially in patients >14 yrs old) (85%)
- V1-V3 QRS widening
- Sudden VT episodes with a LBBB morphology
- Prolonged S-wave upstroke of 55 ms in V1-3 (95%)
Imaging
Major and minor criteria rely on echo and cardiac MRI
- Echo - hypokinetic and dilated RV, dilation of RVOT
- Cardiac MRI - fibro-fatty change with RV myocardial thinning, RV aneurysms, RV dilatation
Management
- Sotalol is the preferred anti-dysrhythmic
- Manage heart failure in the usual manner
Disposition
- Symptomatic presentation: Admission to cardiology
- Incidental finding: Cardiology follow-up for further risk assessment and possible ICD placement or ablation
References
- Anderson EL. Arrhythmogenic right ventricular dysplasia. Am Fam Physician. 2006 Apr 15;73(8):1391-8.
- Perez Diez D, Brugada J. Diagnosis and Management of Arrhythmogenic Right Ventricular Dysplasia. E-Journal of the ESC Council for Cardiology Practice, European Society of Cardiology 2008.
Authors
Kevin Lu, Melody Ong, Neil Young, Ross Donaldson, Daniel Ostermayer