Subarachnoid hemorrhage
Contents
Background

Defined as hemorrhage into the subarachnoid space (between the arachnoid membrane and the pia mater ). This may occur spontaneously, usually from a ruptured cerebral aneurysm, or may result from head injury.
Epidemiology
The prevalence of SAH in patients presenting with true thunderclap headache is estimated at ~10%. [1]
Risk Factors
- Genetics (polycystic kidney disease, Ehler-Danlos, family history)
- Hypertension
- Atherosclerosis
- Cigarette smoking
- Alcohol
- Age >50
- Cocaine use
- Estrogen deficiency
Etiology of Spontaneous SAH
- Ruptured aneurysm (85%)
- Nonaneurysmal (15%)
- Perimesencephalic hemorrhage (10%) - lower risk of complications
- Other: tumor, coagulopathy, dissection, vasculitis, SCD, venous sinus thrombosis
Traumatic Subarachnoid Hemorrhage
- Differentiate from aneurysmal rupture
- Supportive care with prevention of hypertension, elevated ICP, and vasospasm with PO nimodipine
- Observation and repeat head CT for stable patients
Clinical Features
- Sudden, severe headache that reaches maximal intensity within minutes (97% of cases)
- Sudden onset is more important finding than worst headache
- May be associated with syncope, seizure, nausea/vomiting, meningismus
- Meningismus may not develop until hrs after bleed (blood breakdown → aseptic meningitis)
- Retinal hemorrhage
- May be the only clue in comatose patients
- Sentinel bleed headache 6-20 days before serious SAH in 30-50% of patients
Differential Diagnosis
Intracranial Hemorrhage
- Intra-axial
- Hemorrhagic stroke (Spontaneous intracerebral hemorrhage)
- Traumatic intracerebral hemorrhage
- Extra-axial
- Epidural hemorrhage
- Subdural hemorrhage
- Subarachnoid hemorrhage (aneurysmal intracranial hemorrhage)
Other
- Drug toxicity
- Ischemic Stroke
- Meningitis
- Encephalitis
- Intracranial tumor
- Intracranial hypotension
- Metabolic derangements
- Cerebral venous thrombosis
- Primary headache syndromes (benign thunderclap headache, Migraine, Cluster Headache)
Evaluation
Ottawa SAH Rules[2]
Never has been externally and prospectively validated, authors caution implementation into routine use
- 100% sensitive to rule out SAH (97.1%-100%)
- Can exclude SAH if all of the following are true
- Age < 40
- No Neck pain or stiffness
- No Witnessed LOC
- No onset during exertion
- No Thunderclap symptomatology (max intensity at onset)
- No limited neck flexion on physical exam
If concerned for SAH and CT normal strongly consider LP
Non-Contrast Head CT
| Time from onset of symptoms | Sensitivity of CT |
| <6 hours | ~100%[3] |
| 6-12 hours | 98% |
| 12-24 hours | 93%[4] |
| 24 hours - 5 days | <60% |
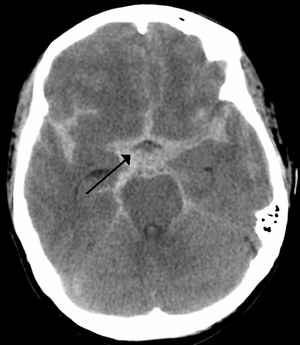
- SAH due to aneurysm - look in cisterns (esp. suprasellar cistern)
- SAH due to trauma - look at convexities of frontal and temporal cortices
Lumbar Puncture
- Elevated RBC count that does not decrease from tube one to four
- Note: decreasing RBCs in later tubes can occur in SAH; only reliable if RBC count in final tube is nl
- Opening pressure >20 (60% of patients)
- Can help differentiate from a traumatic tap (opening pressure expected to be normal)
- Elevated opening pressure also seen in cerebral venous thrombosis, IIH
- Xanthrochromia
- May help differentiate between SAH and a traumatic tap
- Takes at least 2hr after bleed to develop (beware of false negative if measure early)
- Sn (93%) / Sp (95%) highest after 12hr
- If unable to obtain CSF consider CTA
- CTA also highly sensitive for predicting delayed cerebral ischemia
- If traumatic tap is suspected
- Tube 4 RBC count <500 has negative predictive value of 100% for SAH. Tube 4 RBC decrease of 70% compared to tube 1 excludes a radiographically detectable SAH.[5]
- One study found that >2000 RBCs had a sensitivity of 93% and specificity of 93% for SAH, sensitivity increased to 100% when xanthochromia added.[6]
CT Angiogram
- A CT followed by CTA is an acceptable alternative to CT and LP[7]
- CTA has a 98% sensitivity for aneurysms >3mm
Management
Physiologic derangements, such as hypoxemia, metabolic acidosis, hyperglycemia, BP instability, and fever, can worsen brain injury and has been independently associated with increased M&M, but no studies showing benefit of corrections.
- Avoid hypotension
- Hypertension
- AHA/ASA has no formal recommendations but states that decreasing to SBP <160 is reasonable[8]
- Rapid SBP lowering <140 has been advocated with early research showing improved functional outcome[9], but more recent work has found no difference between SBP <140 and <180[10]
- Ensure appropriate pain control and sedation before adding antihypertensives
- Discontinue/reverse all anticoagulation
- Nimodipine
- Only CCB studied that has been shown to prevent vasospasm (associated with improved neuro outcomes and decreased cerebral infarction)
- Give 60mg q4hr PO or NGT only (never IV) within 96hr of symptom onset. NNT 13 to prevent one poor outcome
- Keep an eye on BP for fluctuations
- Magneisum sulfate
- Controversial; prevents vasospasm acting as NMDA antagonist and a calcium channel blocker; maintain between 2-2.5 mmol/L
- Seizure prophylaxis
- Controversial; 3 day course may be preferable
- Phenytoin, levetiracetam, carbamazepine and phenobarb. Phenytoin can be associated with worse neurologic & cognitive outcome
- Glucocorticoid therapy
- Controversial; evidence suggests is neither beneficial nor harmful
- Glycemic control
- Controversial; consider sliding scale if long patient stay in ED while awaiting ICU bed
- Keep head of bed elevated
- Aneurysm treatment
- Surgical clipping and endovascular coiling are definitive treatment
- Antifibrinolytic - Controversial; if delayed aneurysmal treatment, consider short term therapy (<72 hrs) with TXA or aminocaproic acid
Intubation
- Consider neuroprotective intubation
- Ensure patient is pain-free for post-intubation sedation
- Propofol with fentanyl
- Try to prioritize pain control with fentanyl
AHA Aneurysmal SAH BP Guidelines[12]
- No well-controlled studies exist that answer whether BP control influences rebleeding
- BP should be controlled to balance the risk of stroke, hypertension-related rebleeding, and maintenance of cerebral perfusion pressure (Class I, Level of Evidence B).
- Nicardipine, labetalol, and esmolol are appropriate choices for BP control (Sodium nitroprusside may raise intracranial pressure and cause toxicity with prolonged infusion and should be avoided)
Disposition
- Admit
Complications
Rebleeding
- Risk is highest within first 24 hours (2.5-4%), particularly within first 6 hours
- Usually diagnosed by CT after acute deterioration in neuro status
- Only aneurysm treatment is effective in preventing rebleeding
Vasospasm
- Leading cause of death and disability after rupture
- Typically begins no earlier than day three after hemorrhage
- Characterized by decline in neuro status
- Aggressive treatment can only be started after aneurysm has been treated
- treatment for symptomatic vasospasm: Triple-H therapy (hemodilution + induced hypertension (pressors) + hypervolemia), balloon angioplasty, or intra-arterial vasodilatorsScript errorScript error[citation needed]
- Studies have not provided strong evidence of benefit Triple-H therapyScript errorScript error[citation needed]
Cardiac abnormalities
Most likely related to the release of catecholamines due to hypoperfusion of hypothalamus
- Ischemia
- Elevated troponin (20-40% of cases)
- ST segment depression
- Rhythm disturbances
- QT prolongation
- Deep, symmetric TWI
- Prominent U waves
Hydrocephalus
- Consider ventricular drain placement for deteriorating LOC + no improvement within 24hr
Hyponatremia
- Hyponatremia is seen in 10%-40% of the patients with subarachnoid hemorrhage who are admitted to the ICU.[13]
- Cerebral Salt Wasting and SIADH are the two most common causes[14]
Prognosis
Hunt and Hess
Subjective terminology, but good interobserver variability
| Grade | Description | Survival Rate |
| 0 | Unruptured aneurysm | - |
| 1 | Asymptomatic or mild HA and slight nuchal rigidity | 70% |
| 1a | No acute meningeal/brain reaction, with fixed neurological def | - |
| 2 | Moderate to severe HA, stiff neck, no neurologic deficit except CN palsy | 60% |
| 3 | Mild mental status change (drowsy or confused), mild focal neurologic deficit | 50% |
| 4 | Stupor or moderate to severe hemiparesis | 20% |
| 5 | Coma or decerebrate rigidity | 10% |
- Grade 1 or 2 have curable disease
- Add one grade for serious systemic disease (hypertension, DM, severe atherosclerosis, COPD)
World Federation of Neurosurgical Societies (WFNS)
Objective terminology, and fair interobserver variability
| Grade | GCS | Focal neurological deficit |
|---|---|---|
| 1 | 15 | Absent |
| 2 | 13–14 | Absent |
| 3 | 13–14 | Present |
| 4 | 7–12 | Present or absent |
| 5 | <7 | Present or absent |
Other scales are also available, including the Ogilvy and Carter scale (comprehensive, yet complex), and the Fisher scale or Claassen grading system (vasospasm index risk).
Note: First-degree relatives are at 2-5 fold increase in SAH, so screening is considered on individual basis.
See Also
External Links
References
- ↑ Dubosh NM et al. Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Stroke 2016. PMID: 26797666
- ↑ Ottawa SAH Rule JAMA. 2013 Sep 25;310(12):1248-55. doi: 10.1001/jama.2013.278018
- ↑ Perry JJ, et al. Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: prospective cohort study. BMJ. 2011; 343:d4277.
- ↑ van Gijn J and van Dongen KJ. The time course of aneurysmal haemorrhage on computed tomograms. Neuroradiology. 1982; 23:153–156.
- ↑ Gorchynski J, Oman J, and Newton T. Interpretation of traumatic lumbar punctures in the setting of possible subarachnoid hemorrhage: who can be safely discharged? Cal J Emerg Med. 2007; 8(1): 3–7.
- ↑ Perry JJ, Alyahya B, Sivilotti MLA, et al. Differentiation between traumatic tap and aneurysmal subarachnoid hemorrhage: prospective cohort study. BMJ : British Medical Journal. 2015;350:h568.
- ↑ Walsh B, Vilke GM, Coyne CJ. Clinical Guidelines for the Emergency Department Evaluation of Subarachnoid Hemorrhage. Meurer WJ, JEM. 2016; 50(4) 696-701.
- ↑ Connolly ES Jr, Rabinstein AA, Carhuapoma JR, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012; 43(6):1711-1737.
- ↑ Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013; 368:2355-2365.
- ↑ Qureshi AI, Palesch YY, Barsan WG, et al. Intensive Blood-Pressure Lowering in Patients with Acute Cerebral Hemorrhage. N Engl J Med. 2016; 1-11. [Epub ahead of print].
- ↑ Bucher J and Koyfman A. Intubation of the neurologically injured patient. J Emerg Med. 2016; 49:920-927.
- ↑ Bederson J. et al. Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage: A Statement for Healthcare Professionals From a Special Writing Group of the Stroke Council, American Heart Association. Stroke. 2009;40:994-1025 PDF
- ↑ Woo, M.H, Kale-Pradhan, P.B. Fludrocortisone in the treatment of subarachnoid hemorrhage-induced hyponatremia. Annals of Pharmacotherapy. 1997. 31, 637–639.
- ↑ Albanese, A. et al. . Management of hyponatremia in patients with acute cerebral insults. Archives of Disease in Childhood, 85. (2001). 246–251.