We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Transient ischemic attack
From WikEM
(Redirected from TIA)
Contents
Background
- Abbreviation: TIA
- New Definition: a brief episode of neurologic dysfunction caused by focal brain or retinal ischemia, with clinical symptoms typically lasting less than one hour, and without evidence of acute infarction. [1]
- Should be viewed as analogous to unstable angina
- Classic Definition: A sudden, focal neurologic deficit that lasts for less than 24 hours, is presumed to be of vascular origin, and is confined to an area of the brain or eye perfused by a specific artery[1]
- Since 15% of strokes are preceded by TIA, timely eval of high risk conditions like Atrial Fibrillation and Carotid Stenosis is important
Clinical Features
- Focal weakness (Paralysis or paresis of the face, arm, or leg and typically unilateral)
- Dysarthria or dysphasia or aphasia
- Vision changes (Field deficits, blindness, or diplopia)
- Changes in balance or coordination
Differential Diagnosis
Stroke-like Symptoms
- Stroke
- Seizures/postictal paralysis (Todd paralysis)
- Syncope
- Hypoglycemia
- Hyponatremia
- Meningitis/encephalitis
- Hyperosmotic Coma
- Labyrinthitis
- Drug toxicity
- Lithium, phenytoin, carbamazepine
- Bell's Palsy
- Complicated migraine
- Meniere Disease
- Demyelinating disease (MS)
- Conversion disorder
- Transient global amnesia
Evaluation
Stroke Work-Up
- Labs
- POC glucose
- CBC
- Chemistry
- Coags
- Troponin
- T&S
- ECG
- In large ICH or stroke, may see deep TWI and prolong QT, occ ST changes
- Head CT (non-contrast)
- Also consider:
- CTA brain and neck (to check for large vessel occlusion for potential thrombectomy)
- Pregnancy test
- CXR (if infection suspected)
- UA (if infection suspected)
- Utox (if ingestion suspected)
MR Imaging (for Rule-Out CVA or TIA)
- MRI Brain with DWI (without contrast) AND
- Cervical vascular imaging (ACEP Level B in patients with high short-term risk for stroke):[5]
- MRA brain (without contrast) AND
- MRA neck (without contrast)
- May instead use Carotid CTA or US (Carotid US slightly less sensitive than MRA)[6] (ACEP Level C)
Management
- Little acute management (given normally resolution of symptoms)
- Consider aspirin (once hemorrhage ruled-out)
Disposition
ABCD2 Score[7]
- Risk of stroke at 2d, 7d, and 90d from TIA
- Although prognostic, evidence-based admission thresholds have not been determined
- None with score <3 had CVA within one week in study
Scoring
- Age >60yr (1 pt)
- BP (SBP >140 OR diastolic >90) (1 pt)
- Clinical Features
- Isolated speech disturbance (1 pt)
- Unilateral weakness (2 pts)
- Duration of symptoms
- 10-59 min (1 pt)
- >60 min (2 pts)
- Diabetes mellitus (1 pt)
| Points | Stroke Risk | Two Days | Seven Days | 90 Days |
| 0-3 | Low | 1.0% | 1.2% | 3.1% |
| 4-5 | Moderate | 4.1% | 5.9% | 9.8% |
| 6-7 | High | 8.1% | 11.7% | 17.8% |
AHA/ASA Guidelines[8]
- Reasonable to hospitalize patients with TIA who present within 72 hr of symptom onset and have:
- ABCD2 score of ≥ 3
- ABCD2 score of 0-2 and uncertainty that diagnostic workup can be completed within 2d as outpatient
- ABCD2 score of 0-2 and other evidence that event was caused by focal ischemia
NSA Guidelines[9]
- Hospitalization for patients with first TIA within past 24-48hr
- Recommended admission for patients with the following:
- Crescendo TIA (more than three TIAs in 72hr period)
- Duration of symptoms >1hr
- Symptomatic carotid stenosis >50%
- Known cardiac source of embolus
- Known hypercoaguable state
- High risk of early stroke after TIA
ACEP Guidelines[5]
- Level B: In adult patients with suspected TIA, do not rely on current existing risk stratification instruments (eg, age, blood pressure, clinical features, duration of TIA and presence of diabetes [ABCD2] score) to identify TIA patients who can be safely discharged from the ED.
- In contrast to the 2009 AHA/ASA recommendations that were based on limited research, the ABCD2 does not sufficiently identify the short-term risk for stroke to use alone as a risk-stratification instrument.
- Multiple other risk-stratification instruments have been evaluated less frequently than the ABCD2 score. None have demonstrated the ability to identify individual patients at sufficiently low short-term risk for stroke to use alone as a risk-stratification instrument.
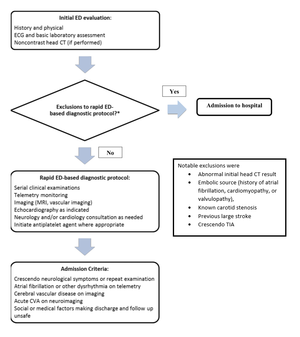
- Level B: A rapid ED based diagnostic protocol can be used to safely identify patients at short-term risk for stroke.
- Study based on observation units and outpatient TIA clinics[10]
External Links
See Also
References
- ↑ 1.0 1.1 Albers GW, et al. The TIA Working Group. Transient ischemic attack: proposal for a new definition. N Engl J Med. 2002; 347:1713–1716.
- ↑ Mullins ME, Schaefer PW, Sorensen AG, Halpern EF, Ay H, He J, Koroshetz WJ, Gonzalez RG. CT and conventional and diffusion-weighted MR imaging in acute stroke: study in 691 patients at presentation to the emergency department. Radiology. 2002 Aug;224(2):353-60.
- ↑ Suarez JI, Tarr RW, Selman WR. Aneurysmal subarachnoid hemorrhage. N Engl J Med. 2006; 354(4):387–396.
- ↑ Douglas VC, Johnston CM, Elkins J, et al. Head computed tomography findings predict short-term stroke risk after transient ischemic attack. Stroke. 2003;34:2894-2899.
- ↑ 5.0 5.1 ACEP Clinical Policy: Suspected Transient Ischemic Attackfull text
- ↑ Nederkoorn PJ, Mali WP, Eikelboom BC, et al. Preoperative diagnosis of carotid artery stenosis. Accuracy of noninvasive testing. Stroke. 2002;33:2003-2008.
- ↑ Johnston SC, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack.Lancet. 2007; 369(9558):283-92.
- ↑ Easton JD, et al. Definition and evaluation of transient ischemic attack. A scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. Stroke. 2009; 40:2276-2293.
- ↑ Johnston SC, et al. National Stroke Association guidelines for the management of transient ischemic attacks. Ann Neurol. 2006; 60(3):301-13.
- ↑ Ross MA, Compton S, Medado P, et al. An emergency department diagnostic protocol for patients with transient ischemic attack: a randomized controlled trial. Ann Emerg Med. 2007;50:109-119