We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Internal hemorrhoid
From WikEM
Contents
Background
- Pathologic state cccurs when internal or external hemorrhoid plexus become engorged, prolapsed, or thrombosed
- Bleeding is usually limited (surface of stool, on toilet tissue, at end of defecation)
- Passage of blood clots requires evaluation for colon lesions
Risk Factors
- Constipation and straining at stool
- Frequent diarrhea
- Older age
- IBD
Clinical Features
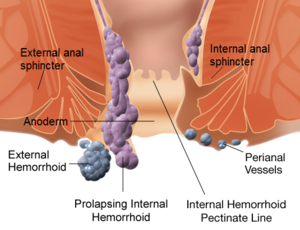
- Occur proximal to dentate line
- Constant in their location: 2-, 5-, and 9-o'clock positions (when patient viewed prone)
- Not readily palpable; best visualized through anoscope
- May be palpable when prolapsed or thrombosed
- Painless bleeding
- Only painful when nonreducible, strangulation of prolapsed hemorrhoid, or thrombosis (these can lead to infection/necrosis)
Differential Diagnosis
Anorectal Disorders
- Anal tags
- Hemorrhoids
- Internal hemorrhoid
- External hemorrhoid
- Cryptitis
- Anal fissure
- Anal fistula
- Anorectal abscess
- Proctitis
- Rectal prolapse
- Rectal foreign body
- Pruritus ani
- Pilonidal cyst
- Constipation
- Condyloma acuminata
- Anal cancer
- Colorectal tumor
- Pedunculated polyp
- Crohn Disease
- Syphilitic fissure
- GC/Chlamydia
Lower gastrointestinal bleeding
- Upper GI Bleeding
- Diverticular disease
- Vascular ectasia
- Inflammatory bowel disease
- Infectious colitis
- Mesenteric Ischemia
- Meckel's diverticulum
- Malignancy / polyps
- Hemorrhoids
- Internal hemorrhoid
- External hemorrhoid
- Aortoenteric fisulta
- Rectal foreign body
- Rectal ulcer (HIV, Syphilis, STI)
- Anal fissure
Evaluation
Internal hemorrhoid chart
| Grade | Description | Diagram | Picture |
|---|---|---|---|
| I |
|
 |

|
| II |
|
 |

|
| III |
|
 |

|
| IV |
|
 |

|
Management
- Conservative treatment
- Indicated for mild to moderate symptomatic patients with grade 1 to grade 3 hemorrhoids
- Stool softeners (psyllium), high-fiber diet, topical analgesics
- Avoid laxatives causing liquid stool (can lead to cryptitis and anal sepsis)
- Sitz bath 15min TID and after each bowel movement (decreases sphincter pressure)
- Outpatient surgical referral
- Prolapsed hemorrhoid in patient with minimal symptoms can be manually reduced
- Emergent surgical consultation and intervention is indicated for:
- Continued and severe bleeding
- Incarceration and/or strangulation (grade 4 hemorrhoids)
- Intractable pain
Prolapse
- When prolapse occurs may develop mucous discharge and pruritus ani
- If prolapse cannot be reduced progressive edema and strangulation may result
- Other complications: severe bleeding, thrombosis, infarction, gangrene, sepsis
Disposition
- Generally may be discharged (unless need for surgical intervention)