We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Le Fort fractures
From WikEM
Contents
Background
- LeFort I fractures are isolated to the lower face
- Type II and III injuries[1]
- Associated with cribriform plate disruption and CSF rhinorrhea
Classification
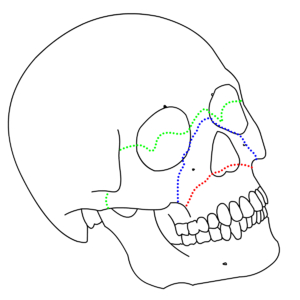
Le Fort I
- Transverse fracture separating body of maxilla from pterygoid plate and nasal septum[1]
- Only hard palate and teeth move (when rock hard palate while stabilizing forehead)
- Stable fracture
Le Fort II
- Pyramidal fracture through central maxilla and hard palate
- Movement of hard palate and nose occurs, but not the eyes
- Can be stable or unstable fracture
Le Fort III
- Craniofacial dysjunction (fracture through frontozygomatic sutures, orbit, nose, ethmoids)
- Entire face shifts with globes held in place only by optic nerve)
- Dish face deformity on lateral view
- Unstable fracture
Le Fort IV
- Le Fort III plus involvement of frontal bone
- Unstable fracture
Differential Diagnosis
Maxillofacial Trauma
- Le Fort fractures
- Skull fracture (peds)
- Auricular hematoma
- Nasal fracture
- Zygomatic arch fracture
- Zygomaticomaxillary (tripod) fracture
- Dental trauma
- Mandible fracture
Orbital trauma
Acute
- Ruptured Globe^
- Corneal Abrasion
- Ocular foreign body
- Conjunctival laceration
- Caustic Keratoconjunctivitis^^
- Subconjunctival hemorrhage
- Traumatic iritis
- Traumatic hyphema
- Retinal detachment
- Retrobulbar hemorrhage/hematoma
- Traumatic mydriasis
- Orbital fracture
- Frontal sinus fracture
- Naso-ethmoid fracture
- Inferior orbial wall fracture
- Medial orbital wall fracture
Subacute/Delayed
Management
- Airway protection
- Consider awake intubation (eg, ketamine) if need airway; if possible do not paralyze a Le Fort for intubation or you may be forced into a crash surgical airway
- Prepare for surgical airway
- CT Face
- Control hemorrhage with nasal and oral packing if needed
- Admit for IV antibiotics and surgery