We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
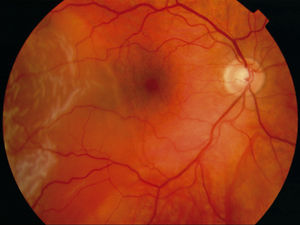
Retinal detachment
From WikEM
Contents
Background

- Average age of onset ~55
Types
- Rhegmatogenous (rhegma means "tear")
- As vitreous separates from retina the traction creates a hole in retina
- Fluid goes through the hole and peels the retina off like wallpaper
- As vitreous separates from retina the traction creates a hole in retina
- Exudative
- Fluid accumulates beneath the retina without a retinal tear
- Associated with neoplasm, inflammatory conditions, hypertension, preeclampsia
- Tractional
- Acquired fibrocellular bands in the vitrous contract and detach the retina
- Associated with DM, sickle cell, trauma
- Distinguish between mac-off and mac-on
- Other risk factors:
- Aging
- Previous retinal detachment
- Family history of retinal detachment
- Extreme myopia
- Eye surgery, cataract removals
Clinical Features
- Abrupt onset of new "floaters" or flashes of light
- Vitreous tugs on the retina before separation
- Visual acuity loss (filmy, cloudy, or curtain-like) or visual field loss
- May be mild or dramatic
Differential Diagnosis
Acute Vision Loss (Noninflamed)
- Arteritic anterior ischemic optic neuropathy
- Amaurosis fugax
- Central retinal artery occlusion (CRAO)†
- Central retinal vein occlusion (CRVO)†
- High altitude retinopathy
- Open-angle glaucoma
- Optic neuritis
- Posterior Reversible Encephalopathy Syndrome (PRES)
- Retinal detachment†
- Temporal arteritis†
- Traumatic optic neuropathy
- Vitreous hemorrhage
- Stroke†
†Emergent Diagnosis
Acute onset flashers and floaters
- Ocular causes
- Floaters and/or flashes
- Posterior Vitreous Detachment
- Retinal tear or Retinal Detachment
- Posterior Uveitis
- Predominantly floaters
- Vitreous Hemorrhage secondary to proliferative retinopathy
- Sympathetic ophthalmia
- Predominantly flashes
- Oculodigital stimulation
- Rapid eye movements
- Neovascular age-related macular degeneration
- Floaters and/or flashes
- Nonocular causes
- Migraine aura (classic)
- Migraine aura (acephalgicmigraine)
- Occipital lobe disorders
- Postural hypotension
Evaluation

- Examination
- Visual acuity and visual fields
- Fundoscopic exam with dilation
- [Ocular ultrasound]]
Management
- Urgent ophtho referral within 24hr (pneumatic retinopexy, scleral buckle, or vitrectomy)[1]
- In macular off retinal detachment, visual acute is significantly decreased if reattachment does not occur within 6 days. [2]
- Position patient relative to area of retinal detachment so retina lies flat:
- Superior detachment = lay patient's head in supine position
- Inferior detachment = elevate head up
- Different from face-down recovery position after pneumatic retinopexy (so that bubble covers retinal break)
- May know where retinal detachment is by a couple of clues:
- Good fundoscopy
- US beam orientation
- Visual Field Defects examples[3]:
- Superior detachment may have inferior visual field defect
- Temporal detachment may have nasal visual field defect
See Also
References
- ↑ Illinois Retina and Eye Associates. Retinal Detachment. 2009. http://www.illinoisretinainstitute.com/index.php?p=1_11.
- ↑ Diederen R et al: Scleral buckling surgery after macula-off retinal detachment: Worse visual outcome after more than 6 days. Ophthalmology 2007; 114:705-709
- ↑ Gariano RF and Kim CH. Evaluation and Management of Suspected Retinal Detachment. Am Fam Physician. 2004 Apr 1;69(7):1691-1699.