We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Systemic lupus erythematosus
From WikEM
(Redirected from Lupus)
Contents
Background
- Autoimmune disorder affecting all systems
- Also consider drug induced lupus
Epidemiology
- Female:Male 10:1
- Peak in 20s-30s
- More common in Black patients
Clinical Features
SLICC Classification Criteria 2012 [1] Requirements: >4 of the following criteria (at least 1 clinical and 1 laboratory) OR biopsy proven lupus nephritis with positive ANA or Anti-dsDNA
- Clinical criteria
- Malar rash, bullous lupus, photosensitivity
- Discoid rash, hypertrophic lupus
- Oral ulcers or nasal ulcers
- Non-scarring alopecia
- Synovitis
- Serositis
- Nephritis
- Cerebritis, myelitis, neuropathy
- Hemolytic anemia
- Leukopenia or lymphopenia
- Thrombocytopenia
- Immunological criteria
- ANA
- Anti-dsDNA
- Anti-Sm
- Antiphospholipid antibody
- Low complement C3, low C4
- Direct Coombs' test in the absence of haemolytic anaemia
Organ system affected:
- Cardiopulmonary
- Pneumonia
- Cover for Listeria and Pseudomonas
- CAD
- More common and more complications post-PCI
- PE
- Pericarditis
- Endocarditis
- Infectious and Libman-Sachs
- Pneumonia
- Neuropsychiatric/Altered mental status
- Non-convulsive status epilepticus
- CNS vasculitis
- Stroke
- Encephalitis
- Meningitis
- Musculoskeletal
- Arthritis
- Usually symmetric
- Consider septic arthritis if there is a single inflamed joint
- Cover for Salmonella in addition to standard coverage
- Arthritis
- GI
- Lupus enteritis (mesenteric vasculitis)
- Most common cause of acute abdominal pain
- Pancreatitis
- PUD
- Lupus enteritis (mesenteric vasculitis)
- Dermatologic
- Malar rash across bridge of nose
- Discoid rash, erythematous with scale
- Treat with topical 1% hydrocortisone
- Renal
- Usually a nephritis
- Can cause a glomerulonephrosis
Differential Diagnosis
- Rheumatoid arthritis
- Sjogren's syndrome
- Dermatomyositis
- Polymyositis
- Stevens-Johnson syndrome
- Toxic Epidermal Necrolysis
- Septic Arthritis
- Lyme Disease
- Vasculitis
- Acute Rheumatic Fever
- Toxic Shock Syndrome
- TTP
- ITP
- DIC
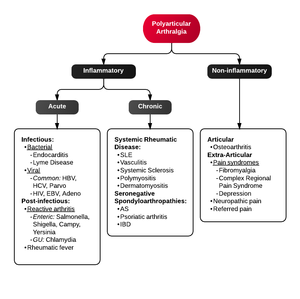
Polyarthritis
- Fibromyalgia
- Juvenile idiopathic arthritis
- Lyme disease
- Osteoarthritis
- Psoriatic arthritis
- Reactive poststreptococcal arthritis
- Rheumatoid arthritis
- Rheumatic fever
- Serum sickness
- Systemic lupus erythematosus
- Serum sickness–like reactions
- Viral arthritis
Causes of Glomerulonephritis
- Poststreptococcal glomerulonephritis
- Hemolytic-uremic syndrome
- Henoch-Schonlein purpura
- IgA nephropathy
- Lupus nephritis
- Alport syndrome
- Goodpasture syndrome
Evaluation
Undiagnosed
- CBC
- Chem 10
- Urine pregnancy
- ANA
- ESR
- Urinalysis
- Bedside echo if ill or hypotensive
- (Consider anti-DNA, anti-Smith, anti-Nuclear, anti-phospholipid, C3,C4, direct Coombs')
Flare
- Bedside echo if ill or hypotensive
- CBC
- Chem
- Urinalysis
- Urine pregnancy
- As directed by organ system involved
Drug Induced Lupus
- Anti-histone-Ab positive 95% of the time
- Make sure to review medications
- High risk:
- Procainamide (antiarrhythmic)
- Hydralazine (antihypertensive)
- Moderate to low risk:
- Infliximab anti (TNF-α)
- Etanercept anti (TNF-α)
- Isoniazid (antibiotic)
- Minocycline (antibiotic)
- Pyrazinamide (antibiotic)
- Quinidine (antiarrhythmic)
- D-Penicillamine (anti-inflammatory)
- Carbamazepine (anticonvulsant)
- Oxcarbazepine (anticonvulsant)
- Phenytoin (anticonvulsant)
- Propafenone (antiarrhythmic)
- Chlorpromazine (antipsychotic)
- High risk:
Fever in SLE
- Must differentiate disease activity (flare) from infection
Risk Factors for Infection [2]
- Neutropenia/Lymphopenia
- Hypocomplementemia
- Immunosuppressive therapy (especially Azathioprine [3])
Studies
Management
- Inflammatory complications
- Methylprednisolone 1-2mg/kg in most cases
- Infectious
- Stress dose steroids with hydrocortisone 100mg IV Q8hr if on or recently on steroids
- Dermatologic
- Hydrocortisone 1% cream
- If drug induced lupus, stop medication and consider alternative
Disposition
- Suspected new diagnosis can have out patient workup if well appearing
- Mild flairs can have expedited out patient management
- Musculoskeletal symptoms can usually be managed as out patients
- Chest pain requires urgent ACS evaluation
- Infections usually require admission for antibiotics and systemic corticosteroids
See Also
- Arthritis
- Fever and Rash
- Lupus Anticoagulant
- Pericarditis
- Pericardial Effusion and Tamponade
- Acute Renal Failure
- Adrenal Crisis
References
- ↑ Lisnevskaia L, et al. Systemic Lupus Erythematosus. Lancet. 2014 May 29. Epub ahead of print.
- ↑ Cuchacovich, R., & Gedalia, A. (2009). Pathophysiology and clinical spectrum of infections in systemic lupus erythematosus. Rheumatic diseases clinics of North America, 35(1), 75–93. doi:10.1016/j.rdc.2009.03.003
- ↑ Zhou, W. J., & Yang, C.-D. (2009). The causes and clinical significance of fever in systemic lupus erythematosus: a retrospective study of 487 hospitalised patients. Lupus, 18(9), 807–812. doi:10.1177/0961203309103870
- ↑ Kim, H.-A., Jeon, J.-Y., An, J.-M., Koh, B.-R., & Suh, C.-H. (2012). C-reactive protein is a more sensitive and specific marker for diagnosing bacterial infections in systemic lupus erythematosus compared to S100A8/A9 and procalcitonin. The Journal of rheumatology, 39(4), 728–734. doi:10.3899/jrheum.111044
- ↑ Scirè, C. A., Cavagna, L., Perotti, C., Bruschi, E., Caporali, R., & Montecucco, C. (2006). Diagnostic value of procalcitonin measurement in febrile patients with systemic autoimmune diseases. Clinical and experimental rheumatology, 24(2), 123–128.