

Facts about Cleft Lip and Cleft Palate
 ShareCompartir
ShareCompartir
Cleft lip and cleft palate are birth defects that occur when a baby’s lip or mouth do not form properly during pregnancy. Together, these birth defects commonly are called “orofacial clefts”.
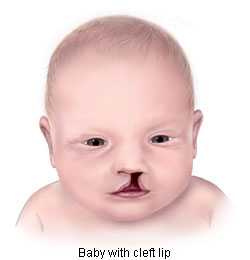
What is Cleft Lip?
The lip forms between the fourth and seventh weeks of pregnancy. As a baby develops during pregnancy, body tissue and special cells from each side of the head grow toward the center of the face and join together to make the face. This joining of tissue forms the facial features, like the lips and mouth. A cleft lip happens if the tissue that makes up the lip does not join completely before birth. This results in an opening in the upper lip. The opening in the lip can be a small slit or it can be a large opening that goes through the lip into the nose. A cleft lip can be on one or both sides of the lip or in the middle of the lip, which occurs very rarely. Children with a cleft lip also can have a cleft palate.
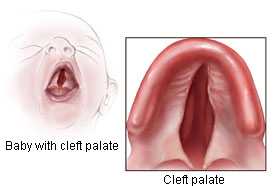
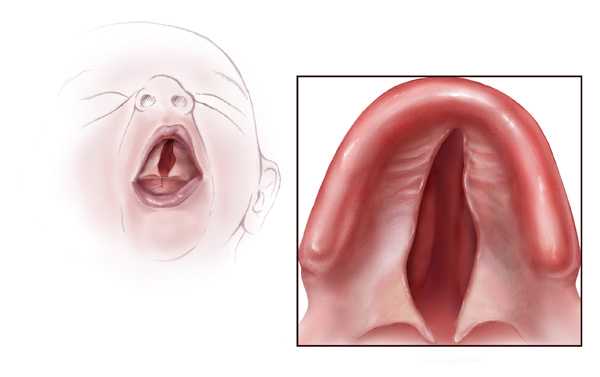
What is Cleft Palate?
The roof of the mouth (palate) is formed between the sixth and ninth weeks of pregnancy. A cleft palate happens if the tissue that makes up the roof of the mouth does not join together completely during pregnancy. For some babies, both the front and back parts of the palate are open. For other babies, only part of the palate is open.
Other Problems
Children with a cleft lip with or without a cleft palate or a cleft palate alone often have problems with feeding and speaking clearly and can have ear infections. They also might have hearing problems and problems with their teeth.
Joshua's Story

Joshua was born with cleft lip and palate. Read his story as well as other stories from families affected by cleft lip and palate »
Occurrence
CDC recently estimated that, each year in the United States, about 2,650 babies are born with a cleft palate and 4,440 babies are born with a cleft lip with or without a cleft palate.1 Isolated orofacial clefts, or clefts that occur with no other major birth defects, are one of the most common types of birth defects in the United States.1 Depending on the cleft type, the rate of isolated orofacial clefts can vary from 50% to 80% of all clefts.2-4
Causes and Risk Factors
The causes of orofacial clefts among most infants are unknown. Some children have a cleft lip or cleft palate because of changes in their genes. Cleft lip and cleft palate are thought to be caused by a combination of genes and other factors, such as things the mother comes in contact with in her environment, or what the mother eats or drinks, or certain medications she uses during pregnancy.
Like the many families of children with birth defects, CDC wants to find out what causes them. Understanding the factors that are more common among babies with a birth defect will help us learn more about the causes. CDC funds the Centers for Birth Defects Research and Prevention, which collaborate on large studies such as the National Birth Defects Prevention Study (NBDPS; births 1997-2011) and the Birth Defects Study To Evaluate Pregnancy exposureS (BD-STEPS; began with births in 2014), to understand the causes of and risks for birth defects, including orofacial clefts.
Recently, CDC reported on important findings from research studies about some factors that increase the chance of having a baby with an orofacial cleft:
- Smoking―Women who smoke during pregnancy are more likely to have a baby with an orofacial cleft than women who do not smoke.2-3
- Diabetes―Women with diabetes diagnosed before pregnancy have an increased risk of having a child with a cleft lip with or without cleft palate, compared to women who did not have diabetes.5
- Use of certain medicines―Women who used certain medicines to treat epilepsy, such as topiramate or valproic acid, during the first trimester (the first 3 months) of pregnancy have an increased risk of having a baby with cleft lip with or without cleft palate, compared to women who didn’t take these medicines.6-7
CDC continues to study birth defects, such as cleft lip and cleft palate, and how to prevent them. If you are pregnant or thinking about becoming pregnant, talk with your doctor about ways to increase your chances of having a healthy baby.
Diagnosis
Orofacial clefts, especially cleft lip with or without cleft palate, can be diagnosed during pregnancy by a routine ultrasound. They can also be diagnosed after the baby is born, especially cleft palate. However, sometimes certain types of cleft palate (for example, submucous cleft palate and bifid uvula) might not be diagnosed until later in life.
Management and Treatment
Services and treatment for children with orofacial clefts can vary depending on the severity of the cleft; the child’s age and needs; and the presence of associated syndromes or other birth defects, or both.
Surgery to repair a cleft lip usually occurs in the first few months of life and is recommended within the first 12 months of life. Surgery to repair a cleft palate is recommended within the first 18 months of life or earlier if possible.8 Many children will need additional surgical procedures as they get older. Surgical repair can improve the look and appearance of a child’s face and might also improve breathing, hearing, and speech and language development. Children born with orofacial clefts might need other types of treatments and services, such as special dental or orthodontic care or speech therapy.4,8
Because children with orofacial clefts often require a variety of services that need to be provided in a coordinated manner throughout childhood and into adolescence and sometimes adulthood, the American Cleft Palate – Craniofacial Association recommends services and treatment by cleft and craniofacial teams.8 Cleft and craniofacial teams provide a coordinated approach to care for children with orofacial clefts. These teams usually consist of experienced and qualified physicians and health care providers from different specialties. Cleft and craniofacial teams and centers are located throughout the United States and other countries. Resources are available to help in choosing a cleft and craniofacial team.
With treatment, most children with orofacial clefts do well and lead a healthy life. Some children with orofacial clefts may have issues with self-esteem if they are concerned with visible differences between themselves and other children. Parent-to-parent support groups can prove to be useful for families of babies with birth defects of the head and face, such as orofacial clefts.
Other Resources
The views of these organizations are their own and do not reflect the official position of CDC.
- American Cleft Palate-Craniofacial Association (ACPA)
ACPA addresses patient care issues and research for all individuals affected by cleft lip and cleft palate. - Cleft Palate Foundation (CPF)
CPF has educational information for parents, families, and professionals, and can make referrals to cleft/craniofacial treatment teams. - Cleft Lip & Palate Foundation of Smiles
Cleft Lip & Palate Foundation of Smiles seeks to provide support for individuals and families with cleft lip and/or palate.
References
- Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, Meyer RE, Anderson P, Mason CA, Collins JS, Kirby RS, Correa A; for the National Birth Defects Prevention Network. Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Research (Part A): Clinical and Molecular Teratology 2010;88:1008-16.
- Little J, Cardy A, Munger RG. Tobacco smoking and oral clefts: a meta-analysis. Bull World Health Organ. 2004;82:213-18.
- Honein MA, Rasmussen SA, Reefhuis J, Romitti P, Lammer EJ, Sun L, Correa A. Maternal smoking, environmental tobacco smoke, and the risk of oral clefts. Epidemiology 2007;18:226–33.
- Yazdy MM, Autry AR, Honein MA, Frias JL. Use of special education services by children with orofacial clefts. Birth Defects Research (Part A): Clinical and Molecular Teratology 2008;82:147-54.
- Correa A, Gilboa SM, Besser LM, Botto LD, Moore CA, Hobbs CA, Cleves MA, Riehle-Colarusso TJ, Waller DK, Reece EA. Diabetes mellitus and birth defects. American Journal of Obstetrics and Gynecology 2008;199:237.e1-9.
- Margulis AV, Mitchell AA, Gilboa SM, Werler MM, Glynn RJ, Hernandez-Diaz S, National Birth Defects Prevention Study. Use of topiramate in pregnancy and risk of oral clefts. American Journal of Obstetrics and Gynecology 2012;207:405.e1-e7.
- Werler MM, Ahrens KA, Bosco JL, Michell AA, Anderka MT, Gilboa SM, Holmes LB, National Birth Defects Prevention Study. Use of antiepileptic medications in pregnancy in relation to risks of birth defects. Annals of Epidemiology 2011;21:842-50.
- American Cleft Palate-Craniofacial Association. Parameters for evaluation and treatment of patients with cleft lip/palate or other craniofacial anomalies. Revised edition, Nov 2009. Chapel Hill, NC. P. 1-34. http://www.acpa-cpf.org/uploads/site/Parameters_Rev_2009.pdf

- Page last reviewed: June 27, 2017
- Page last updated: June 27, 2017
- Content source: