

Facts about Atrioventricular Septal Defect (AVSD)
 ShareCompartir
ShareCompartir
An atrioventricular septal defect (pronounced EY-tree-oh-ven-TRIC-u-lar SEP-tal DEE-fekt) or AVSD is a heart defect affecting the valves between the heart’s upper and lower chambers and the walls between the chambers.
What is Atrioventricular Septal Defect?
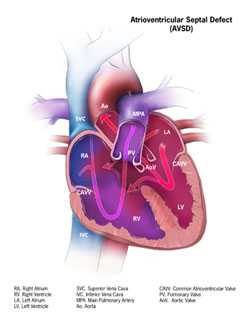
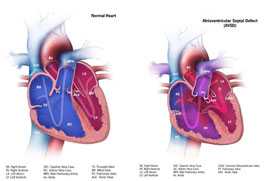
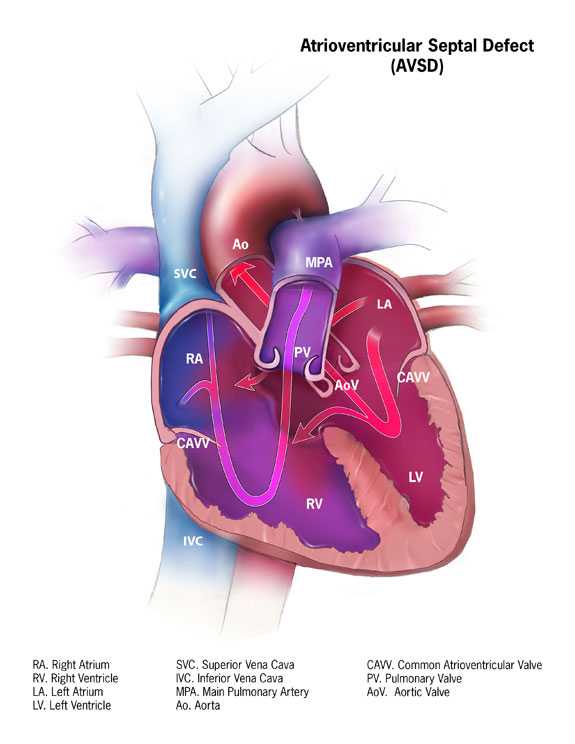
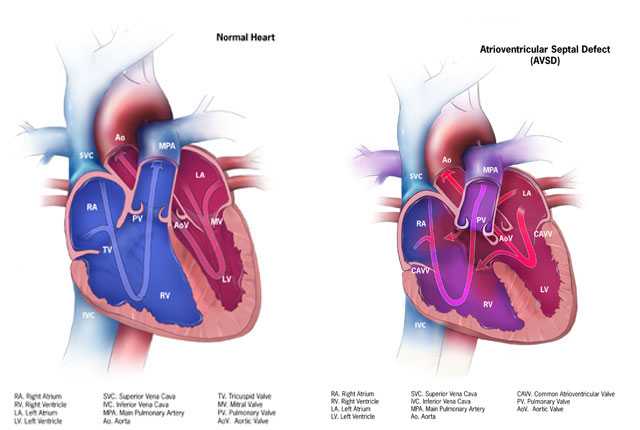
An atrioventricular septal defect (AVSD) is a heart defect in which there are holes between the chambers of the right and left sides of the heart, and the valves that control the flow of blood between these chambers may not be formed correctly. This condition is also called atrioventricular canal (AV canal) defect or endocardial cushion defect. In AVSD, blood flows where it normally should not go. The blood may also have a lower than normal amount of oxygen, and extra blood can flow to the lungs. This extra blood being pumped into the lungs forces the heart and lungs to work hard and may lead to congestive heart failure.
There are two general types of AVSD that can occur, depending on which structures are not formed correctly:
- Complete AVSD
A complete AVSD occurs when there is a large hole in the center of the heart which allows blood to flow between all four chambers of the heart. This hole occurs where the septa (walls) separating the two top chambers (atria) and two bottom chambers (ventricles) normally meet. There is also one common atrioventricular valve in the center of the heart instead of two separate valves – the tricuspid valve on the right side of the heart and the mitral valve on the left side of the heart. This common valve often has leaflets (flaps) that may not be formed correctly or do not close tightly. A complete AVSD arises during pregnancy when the common valve fails to separate into the two distinct valves (tricuspid and mitral valves) and when the septa (walls) that split the upper and lower chambers of the heart do not grow all the way to meet in the center of the heart. - Partial or Incomplete AVSD
A partial or incomplete AVSD occurs when the heart has some, but not all of the defects of a complete AVSD. There is usually a hole in the atrial wall or in the ventricular wall near the center of the heart. A partial AVSD usually has both mitral and tricuspid valves, but one of the valves (usually mitral) may not close completely, allowing blood to leak backward from the left ventricle into the left atrium.
Learn more about how the heart works »
Occurrence
The Centers for Disease Control and Prevention (CDC) estimates that about 2,000 babies (1 in 2,120 babies) are born with AVSD every year in the United States.1
Causes and Risk Factors
The causes of congenital heart defects, such as AVSD, among most babies are unknown. Some babies have heart defects because of changes in their genes or chromosomes. In particular, AVSD is common in babies with Down syndrome, a genetic condition that involves an extra chromosome 21 (also called trisomy 21). Congenital heart defects are also thought to be caused by the combination of genes and other factors that might increase the risk of having a baby with a congenital heart defect, such as things the mother comes in contact with in her environment, what she eats or drinks, or certain medications she uses during pregnancy.
Read more about CDC’s work on causes and risk factors »
Diagnosis
AVSD may be diagnosed during pregnancy or soon after the baby is born.
During Pregnancy
During pregnancy, there are screening tests (also called prenatal tests) to check for birth defects and other conditions. AVSD may be diagnosed during pregnancy with an ultrasound test (which creates pictures of the baby using sound waves), but whether or not the defect can be seen with the ultrasound test depends on the size or type (partial or complete) of the AVSD. The healthcare provider can request a fetal echocardiogram to confirm the diagnosis if AVSD is suspected. A fetal echocardiogram is an ultrasound of the baby’s heart which shows more detail than the routine prenatal ultrasound test. The fetal echocardiogram can show problems with the structure of the heart and how well the heart is working.
After the Baby is Born
During a physical exam of an infant, a complete AVSD may be suspected. Using a stethoscope, a doctor will often hear a heart murmur (an abnormal “whooshing” sound caused by blood flowing through the abnormal hole). However, not all heart murmurs are present at birth. Babies with a complete AVSD usually do show signs of problems within the first few weeks after birth. When symptoms do occur, they may include
- Breathing problems
- Pounding heart
- Weak pulse
- Ashen or bluish skin color
- Poor feeding, slow weight gain
- Tiring easily
- Swelling of the legs or belly
For partial AVSDs, if the holes between the chambers of the heart are not large, the signs and symptoms may not occur in the newborn or infancy periods. In these cases, people with a partial AVSD might not be diagnosed for years.
Symptoms which might indicate that a child’s complete AVSD or partial AVSD is getting worse include
- Arrhythmia, an abnormal heart rhythm. An arrhythmia can cause the heart to beat too fast, too slow, or erratically. When the heart does not beat properly, it can’t pump blood effectively.
- Congestive heart failure, when the heart cannot pump enough blood and oxygen to meet the needs of the body.
- Pulmonary hypertension, a type of high blood pressure that affects the arteries in the lungs and the right side of the heart.
The healthcare provider can request one or more tests to confirm the diagnosis of AVSD. The most common test is an echocardiogram. This is an ultrasound of the heart that can show problems with the structure of the heart, like holes between the chambers of the right and left side of the heart, and any irregular blood flow. An electrocardiogram (EKG), which measures the electrical activity of the heart, chest x-rays, and other medical tests may also be used to make the diagnosis. Because many babies with Down syndrome have an AVSD, all infants with Down syndrome should have an echocardiogram to look for an AVSD or other heart defects.
Treatments
All AVSDs, both partial and complete types, usually require surgery. During surgery, any holes in the chambers are closed using patches. If the mitral valve does not close completely, it is repaired or replaced. For a complete AVSD, the common valve is separated into two distinct valves – one on the right side and one on the left side.
The age at which surgery is done depends on the child’s health and the specific structure of the AVSD. If possible, surgery should be done before there is permanent damage to the lungs from too much blood being pumped to the lungs. Medication may be used to treat congestive heart failure, but it is only a short term measure until the infant is strong enough for surgery.
Infants who have surgical repairs for AVSD are not cured; they might have lifelong complications. The most common of these complications is a leaky mitral valve. This is when the mitral valve does not close all the way so that it allows blood to flow backwards through the valve. A leaky mitral valve can cause the heart to work harder to get enough blood to the rest of the body; a leaky mitral valve might have to be surgically repaired. A child or adult with an AVSD will need regular follow-up visits with a cardiologist (a heart doctor) to monitor his or her progress, avoid complications, and check for other health conditions that might develop as the child gets older. With proper treatment, most babies with AVSD grow up to lead healthy, productive lives.
Reference
- Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, Meyer RE, Anderson P, Mason CA, Collins JS, Kirby RS, & Correa A, for the National Birth Defects Prevention Network. Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol 2010;88:1008-1016.
- Page last reviewed: February 11, 2016
- Page last updated: September 26, 2016
- Content source: