

Circumpolar Health
 ShareCompartir
ShareCompartir
Perspective
People who live in the Arctic and sub-Arctic regions face challenges not usually faced by residents of warmer, more southern environments (1). The cold northern climate keeps people indoors, amplifying the effects of household crowding, smoking and inadequate ventilation on the person-to-person spread of infectious diseases. Residents, governments, and public health authorities of all Arctic countries are increasingly concerned about the spread of zoonotic infections as the climate warms, the emergence of antibiotic resistance among bacterial pathogens, the reemergence of tuberculosis, the entrance of HIV into Arctic communities, the specter of pandemic influenza, and the emergence of new viral pathogens.
In an effort to address these concerns, the International Circumpolar Surveillance (ICS) system was established. ICS is a network of hospitals, public health agencies, and reference laboratories throughout the Arctic linked together to collect, compare, and share uniform laboratory and epidemiological data on infectious diseases of concern and to help develop prevention and control strategies (2). In addition, infectious disease experts have formed work groups to collaborate on research and sentinel surveillance systems are monitoring bacterial and viral pathogens in circumpolar regions.
Program
ICS was established in 1999; its first priority was to share data on invasive bacterial diseases caused by Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis, and groups A and B Streptococcus because: 1) these are diseases of public health importance in Arctic countries, 2) strains of Streptococcus pneumoniae were rapidly acquiring resistance to antibiotics commonly used to treat these infections, 3) most clinical laboratories in Arctic countries routinely culture these pathogens from clinical specimens, and 4) vaccines are available to prevent disease caused by clinically important serotypes of Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis. While no vaccine is currently available for diseases caused by groups A and B Streptococcus, surveillance is important because it allows public health officials to detect outbreaks of group A Streptococcus and to assess the effectiveness of control measures, such as prenatal screening and intrapartum antibiotics for group B Streptococcus.
The establishment of ICS capitalized on existing national infectious disease surveillance systems and long-standing circumpolar collaborative relationships forged through the Arctic Council (www.arctic-council.org) and the International Union for Circumpolar Health (www.iuch.org):
- The Arctic Council is a ministerial forum promoting cooperation and coordination between Arctic Nations on common Arctic concerns. It provides a unique opportunity to partner with Arctic nation ministries of health, non-governmental organizations and indigenous peoples organizations to address health concerns of circumpolar communities. ICS is a project that has been endorsed by the Arctic Council Sustainable Development Working Group.
- The International Union for Circumpolar Health is an association of five national or regional societies with expertise in circumpolar health. ICS is a project within the International Union for Circumpolar Health Infectious Disease Working Group.
Expansion of ICS
ICS has expanded substantially to include multiple countries, additional pathogens, and new programs:
- In 1999, ICS began as a partnership between Alaska and Canada to share data on reported cases of invasive pneumococcal disease from 23 clinical laboratories in Alaska and 14 clinical laboratories in the northern Canadian Arctic including Yukon, Northwest Territory, Nunavut, northern Quebec, and Labrador. Case and culture information was forwarded to the ICS coordinator at CDC’s Arctic Investigations Program (AIP) for analysis, report generation, and dissemination.
- In 1999, ICS also instituted a quality control program among three reference laboratories in Alaska and Canada for serotyping and antimicrobial susceptibility testing of Streptococcus pneumoniae. Each year, participating laboratories exchange panels of pneumococcal isolates for serotyping and susceptibility testing using methods routinely used in each laboratory. Results obtained between each laboratory are compared, discrepancies between results are identified and potential factors contributing to the discrepancies identified.
- In 2000, Greenland joined ICS. Data collection also expanded to include surveillance of other invasive bacterial diseases (Haemophilus influenzae, Neisseria meningitidis, groups A & B Streptococcus) in the U.S. Arctic, northern Canada and Greenland.
- In 2001, Iceland, Norway, and Finland joined ICS and began reporting national pneumococcal disease surveillance and laboratory information to ICS annually. Norway also reports surveillance data for Haemophilus influenzae and Neisseria meningitidis.
- In 2003, Norrbotten, a northern region of Sweden, joined ICS and began reporting invasive diseases caused by Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis, and groups A & B Streptococcus.
- In 2004, the laboratory quality control program was extended to include the Statens Serum Institute in Copenhagen, Denmark.
- In 2005, an ICS quality control exchange program for serotyping of isolates of Haemophilus influenzae and Neisseria meningitidis was implemented. In addition, panels of group A Streptococcus isolates are exchanged between ICS reference laboratories for emm typing.
- In 2006, Vasterbotten, a county in northern Sweden, joined ICS and began sharing regional pneumococcal disease surveillance data.
Governance and Structure of ICS
The priorities and overall direction of ICS are governed by a Steering Committee (see Figure) consisting of two representatives from each participating country, representation from WHO European regional office (Copenhagen), the Indigenous Peoples Secretariat, and Russian Association of Indigenous Peoples of the North. The Steering Committee may identify other infectious diseases of concern and therefore suitable for circumpolar surveillance including sexually transmitted infections, Hepatitis B, HIV/AIDS, and acute respiratory virus diseases such as RSV infections in infants.
Surveillance of invasive bacterial diseases is coordinated by a subcommittee, the Invasive Bacterial Diseases Working Group, chaired by AIP. In 2006, ICS representatives from Canada, Greenland and Alaska met to establish a TB surveillance subgroup of the ICS network to collaboratively address common issues. To date, the ICS-TB Working Group includes jurisdictional representatives from northern Canada, Finland, Greenland, Norway, Sweden, Russian Federation, and the USA (Alaska). The purpose of the working group is to increase knowledge of TB epidemiology related issues in the circumpolar region and to support epidemiologic projects which will provide evidence to inform policy decisions, program design and evaluation in circumpolar jurisdictions. Administration of the working group resides in the Public Health Agency of Canada.
In addition to surveillance activities, circumpolar research working groups can also be formed. To date, a viral hepatitis working group and a Helicobacter pylori working group were formed to promote collaborative research in the Arctic. It is anticipated that as surveillance is implemented for other ICS priority diseases, and research interests develop for other infectious diseases of concern, similar coordinating working groups lead by other partner countries will be established.
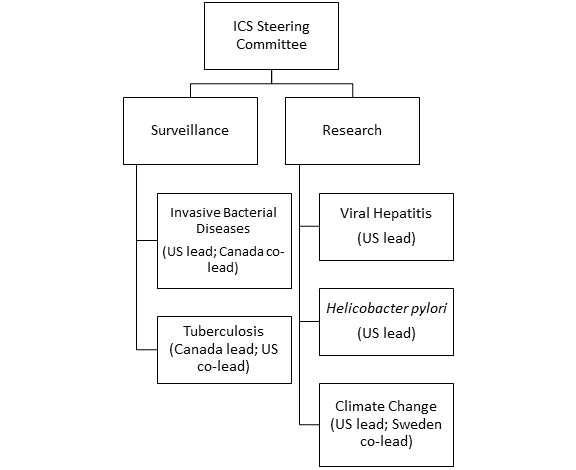
Figure: Structure of the International Circumpolar Surveillance (ICS) system
References
- Parkinson AJ. Climate change and infectious disease: impact on human populations in the Arctic. 2008. In Global climate change and extreme weather events: understanding the contribution to infectious disease emergence (pp. 155-168). Washington, D.C., The National Academies Press.
- Parkinson AJ, Bruce MG, Zulz T. International Circumpolar Surveillance, an Arctic network for the surveillance of infectious diseases. 2008. Emerg Inf Dis 14(1):18-24.
- Page last reviewed: April 1, 2011
- Page last updated: April 1, 2011
- Content source: