

Lesson 1: Introduction to Epidemiology
 ShareCompartir
ShareCompartir
Section 8: Concepts of Disease Occurrence
A critical premise of epidemiology is that disease and other health events do not occur randomly in a population, but are more likely to occur in some members of the population than others because of risk factors that may not be distributed randomly in the population. As noted earlier, one important use of epidemiology is to identify the factors that place some members at greater risk than others.
Causation
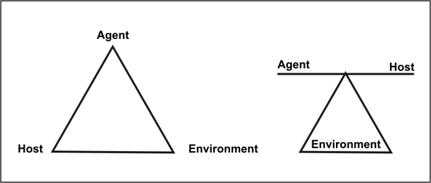
A number of models of disease causation have been proposed. Among the simplest of these is the epidemiologic triad or triangle, the traditional model for infectious disease. The triad consists of an external agent, a susceptible host, and an environment that brings the host and agent together. In this model, disease results from the interaction between the agent and the susceptible host in an environment that supports transmission of the agent from a source to that host. Two ways of depicting this model are shown in Figure 1.16.
Agent, host, and environmental factors interrelate in a variety of complex ways to produce disease. Different diseases require different balances and interactions of these three components. Development of appropriate, practical, and effective public health measures to control or prevent disease usually requires assessment of all three components and their interactions.
Agent originally referred to an infectious microorganism or pathogen: a virus, bacterium, parasite, or other microbe. Generally, the agent must be present for disease to occur; however, presence of that agent alone is not always sufficient to cause disease. A variety of factors influence whether exposure to an organism will result in disease, including the organism's pathogenicity (ability to cause disease) and dose.
Over time, the concept of agent has been broadened to include chemical and physical causes of disease or injury. These include chemical contaminants (such as the L-tryptophan contaminant responsible for eosinophilia-myalgia syndrome), as well as physical forces (such as repetitive mechanical forces associated with carpal tunnel syndrome). While the epidemiologic triad serves as a useful model for many diseases, it has proven inadequate for cardiovascular disease, cancer, and other diseases that appear to have multiple contributing causes without a single necessary one.
Host refers to the human who can get the disease. A variety of factors intrinsic to the host, sometimes called risk factors, can influence an individual's exposure, susceptibility, or response to a causative agent. Opportunities for exposure are often influenced by behaviors such as sexual practices, hygiene, and other personal choices as well as by age and sex. Susceptibility and response to an agent are influenced by factors such as genetic composition, nutritional and immunologic status, anatomic structure, presence of disease or medications, and psychological makeup.
Environment refers to extrinsic factors that affect the agent and the opportunity for exposure. Environmental factors include physical factors such as geology and climate, biologic factors such as insects that transmit the agent, and socioeconomic factors such as crowding, sanitation, and the availability of health services.
Component causes and causal pies
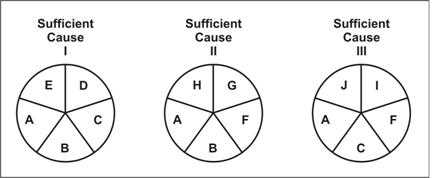
Because the agent-host-environment model did not work well for many non-infectious diseases, several other models that attempt to account for the multifactorial nature of causation have been proposed. One such model was proposed by Rothman in 1976, and has come to be known as the Causal Pies.(42) This model is illustrated in Figure 1.17. An individual factor that contributes to cause disease is shown as a piece of a pie. After all the pieces of a pie fall into place, the pie is complete — and disease occurs. The individual factors are called component causes. The complete pie, which might be considered a causal pathway, is called a sufficient cause. A disease may have more than one sufficient cause, with each sufficient cause being composed of several component causes that may or may not overlap. A component that appears in every pie or pathway is called a necessary cause, because without it, disease does not occur. Note in Figure 1.17 that component cause A is a necessary cause because it appears in every pie.
Figure 1.17 Rothman's Causal Pies
Source: Rothman KJ. Causes. Am J Epidemiol 1976;104:587–592.
The component causes may include intrinsic host factors as well as the agent and the environmental factors of the agent-host-environment triad. A single component cause is rarely a sufficient cause by itself. For example, even exposure to a highly infectious agent such as measles virus does not invariably result in measles disease. Host susceptibility and other host factors also may play a role.
At the other extreme, an agent that is usually harmless in healthy persons may cause devastating disease under different conditions. Pneumocystis carinii is an organism that harmlessly colonizes the respiratory tract of some healthy persons, but can cause potentially lethal pneumonia in persons whose immune systems have been weakened by human immunodeficiency virus (HIV). Presence of Pneumocystis carinii organisms is therefore a necessary but not sufficient cause of pneumocystis pneumonia. In Figure 1.17, it would be represented by component cause A.
As the model indicates, a particular disease may result from a variety of different sufficient causes or pathways. For example, lung cancer may result from a sufficient cause that includes smoking as a component cause. Smoking is not a sufficient cause by itself, however, because not all smokers develop lung cancer. Neither is smoking a necessary cause, because a small fraction of lung cancer victims have never smoked. Suppose Component Cause B is smoking and Component Cause C is asbestos. Sufficient Cause I includes both smoking (B) and asbestos (C). Sufficient Cause II includes smoking without asbestos, and Sufficient Cause III includes asbestos without smoking. But because lung cancer can develop in persons who have never been exposed to either smoking or asbestos, a proper model for lung cancer would have to show at least one more Sufficient Cause Pie that does not include either component B or component C.
Note that public health action does not depend on the identification of every component cause. Disease prevention can be accomplished by blocking any single component of a sufficient cause, at least through that pathway. For example, elimination of smoking (component B) would prevent lung cancer from sufficient causes I and II, although some lung cancer would still occur through sufficient cause III.
 Exercise 1.8
Exercise 1.8
Read the Anthrax Fact Sheet on the following 2 pages, then answer the questions below.
- Describe its causation in terms of agent, host, and environment.
- Agent:
- Host:
- Environment:
- For each of the following risk factors and health outcomes, identify whether they are necessary causes, sufficient causes, or component causes.
Risk Factor/Health Outcome
- _____ Hypertension / Stroke
- _____ Treponema pallidum / Syphilis
- _____ Type A personality / Heart disease
- _____ Skin contact with a strong acid /Burn
Anthrax Fact Sheet
What is anthrax?
Anthrax is an acute infectious disease that usually occurs in animals such as livestock, but can also affect humans. Human anthrax comes in three forms, depending on the route of infection: cutaneous (skin) anthrax, inhalation anthrax, and intestinal anthrax. Symptoms usually occur within 7 days after exposure.
Cutaneous: Most (about 95%) anthrax infections occur when the bacterium enters a cut or abrasion on the skin after handling infected livestock or contaminated animal products. Skin infection begins as a raised itchy bump that resembles an insect bite but within 1–2 days develops into a vesicle and then a painless ulcer, usually 1–3 cm in diameter, with a characteristic black necrotic (dying) area in the center. Lymph glands in the adjacent area may swell. About 20% of untreated cases of cutaneous anthrax will result in death. Deaths are rare with appropriate antimicrobial therapy.
Inhalation: Initial symptoms are like cold or flu symptoms and can include a sore throat, mild fever, and muscle aches. After several days, the symptoms may progress to cough, chest discomfort, severe breathing problems and shock. Inhalation anthrax is often fatal. Eleven of the mail-related cases were inhalation; 5 (45%) of the 11 patients died.
Intestinal: Initial signs of nausea, loss of appetite, vomiting, and fever are followed by abdominal pain, vomiting of blood, and severe diarrhea. Intestinal anthrax results in death in 25% to 60% of cases.
While most human cases of anthrax result from contact with infected animals or contaminated animal products, anthrax also can be used as a biologic weapon. In 1979, dozens of residents of Sverdlovsk in the former Soviet Union are thought to have died of inhalation anthrax after an unintentional release of an aerosol from a biologic weapons facility. In 2001, 22 cases of anthrax occurred in the United States from letters containing anthrax spores that were mailed to members of Congress, television networks, and newspaper companies.
What causes anthrax?
Anthrax is caused by the bacterium Bacillus anthracis. The anthrax bacterium forms a protective shell called a spore. B. anthracis spores are found naturally in soil, and can survive for many years.
How is anthrax diagnosed?
Anthrax is diagnosed by isolating B. anthracis from the blood, skin lesions, or respiratory secretions or by measuring specific antibodies in the blood of persons with suspected cases.
Is there a treatment for anthrax?
Antibiotics are used to treat all three types of anthrax. Treatment should be initiated early because the disease is more likely to be fatal if treatment is delayed or not given at all.
How common is anthrax and where is it found?
Anthrax is most common in agricultural regions of South and Central America, Southern and Eastern Europe, Asia, Africa, the Caribbean, and the Middle East, where it occurs in animals. When anthrax affects humans, it is usually the result of an occupational exposure to infected animals or their products. Naturally occurring anthrax is rare in the United States (28 reported cases between 1971 and 2000), but 22 mail-related cases were identified in 2001.
Infections occur most commonly in wild and domestic lower vertebrates (cattle, sheep, goats, camels, antelopes, and other herbivores), but it can also occur in humans when they are exposed to infected animals or tissue from infected animals.
How is anthrax transmitted?
Anthrax can infect a person in three ways: by anthrax spores entering through a break in the skin, by inhaling anthrax spores, or by eating contaminate, undercooked meat. Anthrax is not spread from person to person. The skin (“cutaneous”) form of anthrax is usually the result of contact with infected livestock, wild animals, or contaminated animal products such as carcasses, hides, hair, wool, meat, or bone meal. The inhalation form is from breathing in spores from the same sources. Anthrax can also be spread as a bioterrorist agent.
Who has an increased risk of being exposed to anthrax?
Susceptibility to anthrax is universal. Most naturally occurring anthrax affects people whose work brings them into contact with livestock or products from livestock. Such occupations include veterinarians, animal handlers, abattoir workers, and laboratorians. Inhalation anthrax was once called Woolsorter's Disease because workers who inhaled spores from contaminated wool before it was cleaned developed the disease. Soldiers and other potential targets of bioterrorist anthrax attacks might also be considered at increased risk.
Is there a way to prevent infection?
In countries where anthrax is common and vaccination levels of animal herds are low, humans should avoid contact with livestock and animal products and avoid eating meat that has not been properly slaughtered and cooked. Also, an anthrax vaccine has been licensed for use in humans. It is reported to be 93% effective in protecting against anthrax. It is used by veterinarians, laboratorians, soldiers, and others who may be at increased risk of exposure, but is not available to the general public at this time.
For a person who has been exposed to anthrax but is not yet sick, antibiotics combined with anthrax vaccine are used to prevent illness.
Sources: Centers for Disease Control and Prevention [Internet]. Atlanta: Anthrax. Available from: http://emergency.cdc.gov/agent/anthrax/ and Anthrax Public Health Fact Sheet, Mass. Dept. of Public Health, August 2002.
References (This Section)
- Rothman KJ. Causes. Am J Epidemiol 1976;104:587–92.
Image Description
Figure 1.16
Description: One model shows agent, host, and environment as having equal influence. The other model shows agent and host as variables that are dependent on each other and on the environment. Return to text.
Figure 1.17
Description: Causal pies are pie charts with each component cause as a slice. Slice A is in each pie. Slice B is only in pies 1 and 2. Slice C is only in pies 1 and 3. Return to text.
- Page last reviewed: May 18, 2012
- Page last updated: May 18, 2012
- Content source: