

Rocky Mountain Spotted Fever
 ShareCompartir
ShareCompartir
Agent
Rickettsia rickettsii
 WHERE FOUND
WHERE FOUND
Although Rocky Mountain spotted fever cases have been reported throughout most of the contiguous U.S., five states (North Carolina, Oklahoma, Arkansas, Tennessee, and Missouri) account for over 60% of RMSF cases.
Rocky Mountain spotted fever has become increasingly common in certain areas of Arizona over the last several years. Between 2003 and 2012 over 250 cases and 19 fatalities occurred. RMSF can be rapidly fatal if not treated within the first 5 days of symptoms. Before tetracycline antibiotics were available, case fatality rates ranged from 20–80%.
INCUBATION PERIOD: 2-14 days
SIGNS AND SYPMTOMS
Localized Stage
- Fever, chills
- Severe headache
- Malaise
- Myalgia
- Gastrointestinal symptoms (nausea, vomiting, anorexia, abdominal pain, diarrhea, abdominal tenderness)
- Cough
- Photophobia
- Focal neurologic deficits, including cranial or peripheral motor nerve paralysis or sudden transient deafness
Maculopapular Rash
- Typically appears 2–5 days after the onset of fever
- Small, flat, pink, non-itchy spots (macules) initially appear on the wrists, forearms, and ankles then spread to the trunk and sometimes palms and soles.
- Rash may not develop until late in the disease process, after treatment should have already begun. Approximately 10% of RMSF patients never develop a rash at all.
- Consider RMSF if other signs and symptoms support a diagnosis, even if a rash is not present.
Petechial Rash
- Red to purple spots (petechiae) are usually not seen until day 6 or later after onset of symptoms.
- Petechial rash is considered a sign of progression to severe disease. Every attempt should be made to begin treatment before petechiae develop.
NOTE: Neurologic symptoms are typically not seen until later in the disease progression and may be prevented with early treatment.
 Confirmation of the diagnosis is based on laboratory testing, but antibiotic therapy should not be delayed in a patient with a suggestive clinical presentation. Antibiotics are less likely to prevent fatal outcome from RMSF if started after day 5 of symptoms.
Confirmation of the diagnosis is based on laboratory testing, but antibiotic therapy should not be delayed in a patient with a suggestive clinical presentation. Antibiotics are less likely to prevent fatal outcome from RMSF if started after day 5 of symptoms.
GENERAL LABORATORY FINDINGS
- Thrombocytopenia
- Mildly elevated hepatic transaminase levels
- Hyponatremia
LABORATORY CONFIRMATION
Antibodies to R. rickettsii are detectable 7–10 days after illness onset. The gold-standard serologic test looks for a four-fold change in antibody titers using indirect immunofluorescence assay (IFA) on paired samples. The first sample should be taken within the first week of illness and the second should be taken 2 to 4 weeks later.
- Demonstration of a four-fold change in IgG-specific antibody titer by indirect immunofluorescence assay (IFA) test in paired serum samples; or
- Detection of DNA in a skin biopsy of rash by polymerase chain reaction (PCR) assay (generally unreliable for acute blood samples).
- Immunohistochemical (IHC) staining of organism from skin or tissue biopsy.
NOTE: IgM antibodies are less specific than IgG antibodies and are more likely to generate false positives. IgM results alone should not be used for laboratory diagnosis.
NOTE: Antibody titers are frequently negative in the first 7–10 days of illness, thus serologic tests may be falsely negative during this time period.
Treatment
Anaplasmosis, ehrlichiosis, and Rocky Mountain spotted fever are treated in the same manner with doxycycline.† Clinical suspicion of any of these diseases is sufficient to begin treatment. Delay in treatment may result in severe illness and even death. The regimens listed below are guidelines only and may need to be adjusted depending on a patient’s age, medical history, underlying health conditions, pregnancy status, or allergies. Consult an infectious disease specialist in cases of pregnancy or documented life-threatening allergies to doxycycline.
| Age Category | Drug | Dosage | Maximum | Duration (Days) |
|---|---|---|---|---|
| Adults | Doxycycline | 100 mg twice per day, orally or IV | 100 mg/dose | Patients should be treated for at least 3 days after the fever subsides and until there is evidence of clinical improvement. Minimum course of treatment is 5-7 days. |
| Children weighing <100 lbs. (45.4 kg) | Doxycycline | 2.2 mg/kg per dose twice per day, orally or IV | 100 mg/dose |
NOTE: Use doxycycline as the first-line treatment for suspected RMSF in patients of all ages. The use of doxycycline to treat suspected RMSF in children is recommended by both the CDC and the American Academy of Pediatrics Committee on Infectious Diseases. Use of antibiotics other than doxycycline increases the risk of patient death. At the recommended dose and duration needed to treat RMSF, no evidence has been shown to cause staining of permanent teeth, even when five courses are given before the age of eight.
References
†Biggs HM, Barton Behravesh C, Bradley KK, et al. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever and other spotted fever group rickettsioses, ehrlichioses, and anaplasmosis — United States. MMWR Recomm Rep 2016; 65 (2); 1-48.
Smithee L, et al. Public health reporting and national notification for spotted fever rickettsiosis [PDF – 96 KB] (including Rocky Mountain spotted fever). Council of State and Territorial Epidemiologists, Infectious Diseases Committee, 2009 Position Statement.
Todd SR, Dahlgren FS, et al. No visible dental staining in children treated with doxycycline for suspected Rocky Mountain spotted fever. J Pediatr, available online 17 March 2015.
Walker DH, Raoult D. Rickettsia ricketsii and other spotted fever group rickettsiae (Rocky Mountain spotted fever and other spotted fevers). In: Mandell GL, Bennett JE, Dolin R, editors. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 6th ed. Philadelphia, PA: Churchill Livingstone; 2005. p. 2287–2295.
Reported Cases of Rocky Mountain Spotted Fever, U.S., 2015
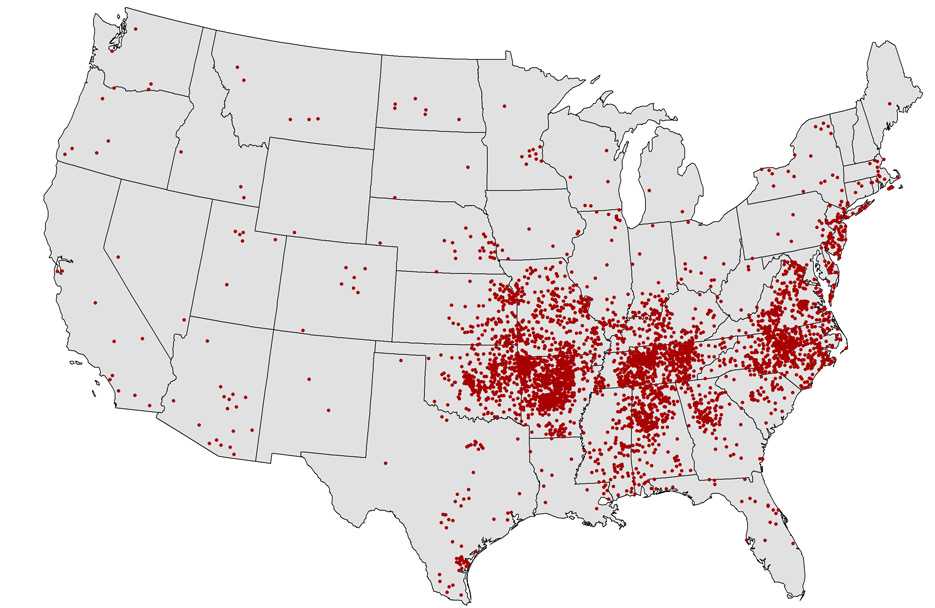
NOTE: Each dot represents one case. Cases are reported from the infected person’s county of residence, not necessarily the place where they were infected.
NOTE: In 2015, no cases of RMSF were reported from Hawaii or Alaska.
- Page last reviewed: October 23, 2014
- Page last updated: February 8, 2017
- Content source: