

Tickborne Relapsing Fever
 ShareCompartir
ShareCompartir
Agent: Borrelia hermsii and other spp.
WHERE FOUND In the U.S., TBRF occurs most commonly in 14 western states: Arizona, California, Colorado, Idaho, Kansas, Montana, Nevada, New Mexico, Oklahoma, Oregon, Texas, Utah, Washington, and Wyoming. Most cases occur in the summer when people vacation and sleep in rodent-infested cabins. However, TBRF can also occur in the winter months when fires started to warm a cabin activate ticks resting in the walls and woodwork.
INCUBATION PERIOD: ~7 days, followed by recurring febrile episodes that last ~3 days and are separated by afebrile periods of ~7 days
SIGNS AND SYPMTOMS
- Headache
- Myalgia
- Chills
- Nausea, vomiting
- Arthralgia
COMMON FINDINGS ON ROUTINE LABORATORY TESTS
- Normal to increased white blood cell count with a left shift
- Mildly increased serum bilirubin
- Mild to moderate thrombocytopenia
- Elevated erthrocyte sedimentation rate
- Slightly prolonged prothrombin time (PT) and partial thromboplastin time (PTT)
LABORATORY DIAGNOSIS
- Observation of Borrelia spirochetes in smears of peripheral blood, bone marrow, or CSF
- Organisms are best detected in blood obtained while a person is febrile
- Serologic testing for TBRF is not standardized and results may vary by laboratory
TREATMENT
- Tetracycline 500 mg every 6 hours for 10 days is the preferred oral regimen for adults. If tetracyclines are contraindicated, an effective alternative is erythromycin 500 mg (or 12.5 mg/kg) every 6 hours for 10 days.
- For CNS involvement, ceftriaxone 2 g per day for 10–14 days is preferred.
- When initiating antibiotic therapy, all patients should be observed during the first 4 hours of treatment for a Jarisch-Herxheimer reaction.
- Acute respiratory distress syndrome requiring intubation has occurred in several patients undergoing TBRF treatment.
References
Centers for Disease Control and Prevention. Acute respiratory distress syndrome in persons with tickborne relapsing fever—Three states, 2004–2005. MMWR 2007;56(41):1073–1076.
Dworkin MS, Schwan TG, et al. Tick-borne relapsing fever. Infect Dis Clin North Am 2008 Sep;22(3):449–8.
Hayes E B and Dennis DT. Relapsing fever. In: Kasper DL, Fauci AS, Longo DL, Braunwald E, Hauser SL, Jameson JL, eds. Harrison’s Principles of Internal Medicine. 16th ed. New York, NY: McGraw-Hill; 2004:991–995.
Cases of Tick-borne Relapsing Fever – United States, 1990 – 2011
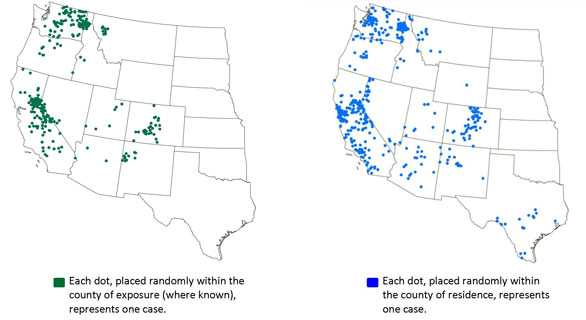
During the years 1990-2011, 483 cases of TBRF were reported in the western U.S., with infections being transmitted most frequently in California, Washington, and Colorado.
- Page last reviewed: October 23, 2014
- Page last updated: October 23, 2014
- Content source: