We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Arsenic toxicity
From WikEM
(Redirected from Arsenic)
Contents
Background
- Heavy metal
- readily absorbed via GI tract and inhalation, poorly via skin
- tasteless and odorless
- organic trioxide form used as chemotherapeutic agent
- trivalent form, As3+, is toxic to over 200 intracellular enzymes
- known carcinogen: skin, lung, other
- ingestion fatal dose: 100-200mg
Sources of Exposure
- Poisoning
- Contaminated drinking water
- Eruptions
- Metal and semiconductor industry
- Wood preservatives
- seafood arsenic (felt to be organic form which is NONTOXIC and cleared from body in few days)
Clinical Features

Acute ingestion
- Garlic smell of breath and tissues
- GI symptoms that can resemble cholera
- Vomiting may be bloody
- "rice water" like diarrhea
- dehydration
- Pulmonary Edema
- Shock
- Rhabdomyolysis
- altered mental status
- Seizure
- coma
- death
- cardiovascular instability
Arsine gas exposure
- hemolysis causing abdominal pain
- hematuria, urine often looks black
- jaundice
- shaking chills
- can lead to altered mental status
- immediately lethal at 250 ppm
Subacute or chronic poisoning
- Anemia
- peripheral neuropathy
- typically symmetric "glove and stocking" distribution
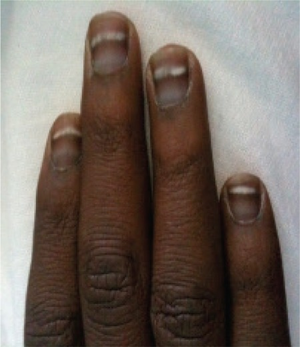
- skin changes
- White lines on the finger nails known as "Mees lines"
- ataxia
- CNS Depression
Differential Diagnosis
Heavy metal toxicity
- Aluminum toxicity
- Antimony toxicity
- Arsenic toxicity
- Barium toxicity
- Bismuth toxicity
- Cadmium toxicity
- Chromium toxicity
- Cobalt toxicity
- Copper toxicity
- Gold toxicity
- Iron toxicity
- Lead toxicity
- Lithium toxicity
- Manganese toxicity
- Mercury toxicity
- Nickel toxicity
- Phosphorous toxicity
- Platinum toxicity
- Selenium toxicity
- Silver toxicity
- Thallium toxicity
- Tin toxicity
- Zinc toxicity
Acute diarrhea
Infectious
- Viral (e.g. rotavirus)
- Bacterial
- Campylobacter
- Shigella
- Salmonella (nontyphi)
- Escherichia coli
- E. coli 0157:H7
- Yersinia enterocolitica
- Vibrio cholerae
- Clostridium difficile
- Parasitic
- Toxin
Noninfectious
- GI Bleed
- Appendicitis
- Mesenteric Ischemia
- Diverticulitis
- Adrenal Crisis
- Thyroid Storm
- Toxicologic exposures
- Antibiotic or drug-associated
- Arsenic toxicity
Watery Diarrhea
- Enterotoxigenic [[E. coli]
- Norovirus (often has prominent vomiting)
- Campylobacter
- Non-typhoidal Salmonella
- Enteroaggregative E. coli (EAEC)
- Enterotoxigenic Bacteroides fragilis
Traveler's Diarrhea
Evaluation
Workup
- Urine arsenic level
- ECG to eval for QT Prolongation in acute exposure
- CBC and retic count, expect hemolytic anemia
- BMP, Mg, phos, Ca, LFTs, CK
- type and screen for possible transfusion in arsine gas exposure
- CXR if respiratory symptoms
- Consider other ingestion labs including acetaminophen and salicylate level in intentional ingestions
Diagnosis
- Urine arsenic level (usual normal level is <50mcg/L); both urine spot test and 24h urine collection
- Lab must differentiate inorganic from organic arsenic (treat for inorganic exposure only)
- Blood arsenic level not helpful (cleared within 2 hrs of exposure)
Management
- supportive care, ABCs, IV, O2, monitor
- removal from exposure
- NO Charcoal if co-ingestion is not suspected - adsorbs poorly to arsenic
- consider Whole Bowel Irrigation if large radiopaque material in GI tract on xray
- airway management and mechanical ventilation if acute inhalation of arsine gas and respiratory distress
- IV fluids
- CHELATION therapy: if severe symptoms present
- Dimercaprol (BAL). 3-5mg/kg IM Q4-6h
Disposition
- admit patient's with significant symptoms
- ED observation and discharge with follow-up for mildly symptomatic