We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Atrial septal defect
From WikEM
Contents
Background
- Many ASDs go undiagnosed in childhood
- From superior to inferior, ASDs occur in[1]:
- Sinus venosus (5%)
- Ostium secundum (75%), ostium primum (15-20%)
- Very rarely coronary sinus ASD
- By 40s, patients may develop symptoms[2]
- Small ASDs < 5 mm in diameter may not generate symptoms
- 5-10 mm defects lead to symptoms in 4th and 5th decade of life
- > 10 mm defects present with symptoms in 3rd decade
- LV stiffness increases as a part of normal aging, impairing left heart diastolic filling[3][4]
- Increases left to right shunt across ASD
- Produces RA and RV volume overload
- May predispose to paradoxical embolus, causing stroke, TIA, acute limb ischemia, mesenteric ischemia, etc.[5]
- Right to left shunt may occur during coughing, for example
- Pulmonary hypertension produces this shunting pattern even at rest
Clinical Features
A patient may be asymptomatic or have any of the following features:
- Dyspnea on Exertion
- CHF
- Palpitations
- Syncope
- Right heart failure
- A. fib
- Stroke (via an embolism)
- Pulmonary hypertension, marker of late disease and increased mortality[6]
- Eisenmenger syndrome
Differential Diagnosis
Congenital Heart Disease Types
- Cyanotic
- Tetralogy of Fallot
- Tricuspid anomalies
- Truncus arteriosus
- Total anomalous pulmonary venous return
- Transposition
- Acyanotic
- VSD
- Atrial septal defect (ASD)
- PDA
- Cor triatriatum
- AV canal
- Pulmonary/aortic stenosis
- Differentiation by pulmonary vascularity on CXR[7]
- Increased pulmonary vascularity
- Decreased pulmonary vascularity
- Tetralogy of Fallot
- Rare heart diseases with pulmonic stenosis
Evaluation
ECG Findings
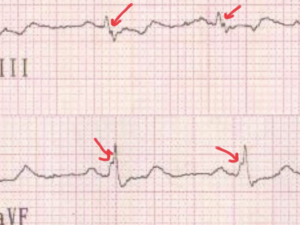
- An ECG may show the “crochetage” pattern (92% specific[8])—a notch near the apex of the R wave in inferior limb leads[9]
- Large notches signify a larger shunt
- Other ECG findings
- (Incomplete right bundle branch block, very sensitive
- 1st degree AV block
- Atrial flutter or atrial fibrillation in ~20% of adults with ASDs requiring surgery[10]
- Right axis deviation (pulmonary hypertension)
Echocardiography
- Subcostal view preferred window, due to interatrial septum perpendicular to echo signal (apical four-chamber is parallel to ASD echo signal)
- Clues to ASD
- Hypermobile interatrial septum
- Abrupt septal irregularity
- RA and/or RV volume overload
- Pulmonary artery dilation
- High pulmonary artery pressures
- TTE with Doppler can demonstrate most shunting
- Agitated saline with Valsalva maneuver to increase right to left shunting is more diagnostic[11]
Management[12]
- Medical management of complications (Afib, pulmonary HTN, etc.)
- Avoid pregnancy and exertional activity in ASD complicated by pulmonary hypertension
- Indications for ASD closure
- Right heart overload with RA or RV enlargement
- Complicated ASDs
Disposition
- Generally unless there is a complication, the septal defect if found incidentally can be evaluated as an outpatient with elective repair
See Also
External Links
References
- ↑ Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease. J Am Coll Cardiol. 2008;52:e143–263.
- ↑ Craig RJ, Selzer A. Natural history and prognosis of atrial septal defect. Circulation. 1968;37:805–15.
- ↑ Fleg JL, Shapiro EP, O’Connor F, Taube J, Goldberg AP, Lakatta EG. Left ventricular diastolic filling performance in older male athletes. JAMA. 1995;273:1371–5.
- ↑ Swinne CJ, Shapiro EP, Lima SD, Fleg JL. Age-associated changes in left ventricular diastolic performance during isometric exercise in normal subjects. Am J Cardiol. 1992;69:823–6.
- ↑ Ward R, Jones D, Haponik EF. Paradoxical embolism. An underrecognized problem. Chest. 1995;108:549–58.
- ↑ Gabriels C, De Meester P, Pasquet A, et al. A different view on predictors of pulmonary hypertension in secundum atrial septal defect. Int J Cardiol. 2014;176:833–40.
- ↑ Knipe K et al. Cyanotic congenital heart diseases. Radiopaedia. http://radiopaedia.org/articles/cyanotic-congenital-heart-disease
- ↑ Heller J, Hagège AA, Besse B, et al. “Crochetage” (notch) on R wave in inferior limb leads: a new independent electrocardiographic sign of atrial septal defect. JAC 1996;27(4):877–82.
- ↑ Heller, J et al. “Crochetage” (Notch) on R wave in inferior limb leads: A new independent electrocardiographic sign of atrial septal defect. J Am Coll Cardiol. 1996;27(4):877-882 full text]
- ↑ Gatzoulis MA, Freeman MA, Siu SC, Webb GD, Harris L. N Engl J Med. 1999 Mar 18; 340(11):839-46.
- ↑ Shub C, Dimopoulos IN, Seward JB, et al. Sensitivity of two-dimensional echocardiography in the direct visualization of atrial septal defect utilizing the subcostal approach: experience with 154 patients. J Am Coll Cardiol. 1983;2:127–35.
- ↑ Martin SS et al. Atrial Septal Defects – Clinical Manifestations, Echo Assessment, and Intervention. Clin Med Insights Cardiol. 2014; 8(Suppl 1): 93–98.
Authors
Kevin Lu, Daniel Ostermayer, Daniel Eggeman, Ross Donaldson, Neil Young