We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Auricular hematoma
From WikEM
(Redirected from Auricular Hematoma)
Contents
Background
- Caused by blunt trauma to external ear
- Associated with contact sports such as boxing, wrestling, etc.
- Separation of perichondrium from underlying cartilage tears the adjoining blood vessels[1]
- Usually occurs on anterior surface, since skin is firmly adherent to cartilage (on posterior ear, there is underlying muscle and adipose is it loosely adherent to cartilage)[2]
- Recurrent hematomas lead to infection and/or cartilage necrosis and neocartilage formation (i.e. "cauliflower ear")
- Goal of treatment is to prevent "cauliflower ear" deformity by draining the hematoma in a timely fashion

Clinical Features
- Gross deformity/swelling to pinna after recent blunt trauma
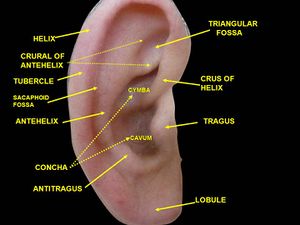
- Loss of typical auricular landmarks/anatomy[3]
- Pain out of proportion[3]
- Hematoma most commonly collects in the scaphoid fossa and the concha
Differential Diagnosis
Ear Diagnoses
- External
- Auricular hematoma
- Cholesteatoma
- Contact dermatitis
- Ear foreign body
- Herpes zoster oticus (Ramsay Hunt syndrome)
- Malignant otitis externa
- Mastoiditis
- Otitis externa
- Otomycosis
- Tympanic membrane rupture
- Internal
- Acute otitis media
- Bullous myringitis
- Chronic otitis media
- Mastoiditis
- Otic barotrauma
- Inner/vestibular
Maxillofacial Trauma
- Le Fort fractures
- Skull fracture (peds)
- Auricular hematoma
- Nasal fracture
- Zygomatic arch fracture
- Zygomaticomaxillary (tripod) fracture
- Dental trauma
- Mandible fracture
Orbital trauma
Acute
- Ruptured Globe^
- Corneal Abrasion
- Ocular foreign body
- Conjunctival laceration
- Caustic Keratoconjunctivitis^^
- Subconjunctival hemorrhage
- Traumatic iritis
- Traumatic hyphema
- Retinal detachment
- Retrobulbar hemorrhage/hematoma
- Traumatic mydriasis
- Orbital fracture
- Frontal sinus fracture
- Naso-ethmoid fracture
- Inferior orbial wall fracture
- Medial orbital wall fracture
Subacute/Delayed
Evaluation
- Clinical diagnosis
Management
Indications for drainage[4]
- Traumatic swelling that deforms pinna
- Within 7 days of trauma
Contraindications
In these cases, refer to ENT due to formation of granulation tissue that may require debridement
- Recurrent or chronic hematomas
- > 7 days from trauma
Procedure
- Perform an auricular block
- Evacuate the clot
- Option 1: Make semi-circle incision inside the inner curvature of the helix or antihelix
- Make incisions along natural auricular crease for cosmesis
- Remove hematoma by milking of the hematoma toward the incision. Suction or curettage may also be helpful
- Use a butterfly hemostat or suture kit needle driver to break up any hematoma that is not easily coming out
- Option 2: Use large-bore needle/syringe to aspirate hematoma[2]
- Needle aspiration generally is not sufficient treatment[3], especially for larger hematomas as clot has usually already formed and cannot be aspirated
- Option 1: Make semi-circle incision inside the inner curvature of the helix or antihelix
- Prevent re-accumulation of hematoma (goal is to close the dead space between perichondrium and cartilage[1]). Multiple methods available:
- Option 1: Compression dressing
- Pack the helix with petroleum jelly-impregnated gauze
- Place regular gauze both in front of and behind the ear
- Circle the head with a compressive wrap
- Generally only moderately successful, and subject to poor compliance (especially with athletes[1])
- Option 2: Suture
- Use fast-absorbing sutures
- Place running or interrupted sutures through cartilage and both anterior and posterior skin of auricle in mattress fashion[2]
- This should reappose the perichondrium
- Consider leaving incision open (with wound edges approximated by mattress sutures) to allow for continued drainage[1]
- Option 3: Bolster sutured in place- combination of the above two methods
- Use non-absorbable 2-0 or 3-0 nylon
- Pack the helix with petroleum jelly impregnated gauze. Place a thick layer of gauze behind the ear
- Perform a running quilt stitch through the anterior gauze, through the pinna, and through the posterior gauze
- Option 1: Compression dressing
- Antibiotics
- Often used by our ENT colleagues in all patients though it is actually only recommended for immunocompromised patients
- Cover pseudomonas and S. aureus- Cipro is the most commonly used
Disposition
- Discharge
- ENT followup in 2-3 days for suture removal or dressing removal and wound check
See Also
References
- ↑ 1.0 1.1 1.2 1.3 Roy S, Smith LP. A novel technique for treating auricular hematomas in mixed martial artists (ultimate fighters). Am J Otolaryngol. 2010 Jan-Feb;31(1):21-4.
- ↑ 2.0 2.1 2.2 Vuyk HD, Bakkers EJ. Absorbable mattress sutures in the management of auricular hematoma. Laryngoscope. 1991 Oct;101(10):1124-6.
- ↑ 3.0 3.1 3.2 Giles WC, Iverson KC, King JD, Hill FC, Woody EA, Bouknight AL. Incision and drainage followed by mattress suture repair of auricular hematoma. Laryngoscope. 2007 Dec;117(12):2097-9.
- ↑ Laybell I et al. Auricular Hematoma Drainage. Aug 7, 2015. http://emedicine.medscape.com/article/82793-overview#a8