We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Blunt neck trauma
From WikEM
Contents
Background
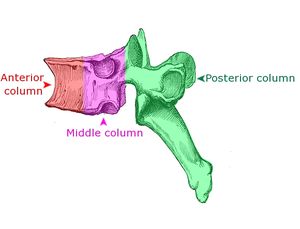
- Suspect vascular damage to cord if discrepancy between neuro deficit and level of spinal column injury
- Spinal cord injury is more likely if anterior (vertebral bodies) AND posterior (spinal canal) columns are disrupted
Clinical Features
- Signs of life-threatening neck or upper thoracic injury (look for TWELVE)
Tracheal deviation, Wounds, External markings, Laryngeal disruption, Venous distention, Emphysema (surgical)
- Features may include signs and symptoms of:
Differential Diagnosis
Blunt Neck Trauma
- Spinal cord trauma
- Vertebral and carotid artery dissection
- Whiplash injury
- Cervical spine fractures and dislocations
- Strangulation
Other
Evaluation
Fracture
NEXUS Cervical Spine Rule
Radiography is not necessary if the patient satisfies ALL of the following low risk criteria:
- No midline cervical tenderness
- No focal neuro deficits
- Normal alertness
- No intoxication
- No painful distracting injury
C-spine imaging should be considered unless the patient meets all of the above low risk criteria[1] [2]
- ^If find injury consider CT C-spine, x-ray rest of spine
Spinal cord trauma
- Neuro exam
Vertebral and Carotid Artery Dissection
The Denver Screening Criteria are divided into risk factors and signs and symptoms
Signs and Symptoms
- Focal neurologic deficit
- Arterial Hemorrhage
- Cervical Bruit or Thrill (<50yo)
- Infarct on Head CT
- Expanding Neck Hematoma
- Neuro exam inconsistent with Head CT
Risk Factors
- Midface Fractures
- Cervical Spine Injuries
- Basilar Skull Fracture
- GCS<8
- Hanging with Anoxic Brain Injury
- Seat belt abrasion or other soft tissue injury of the anterior neck resulting in significant swelling or altered mental status
Pediatrics
- In a small study of 42 patients with a cervical seatbelt sign there were no isolated cerebrovascular injuries. For pediatric patients in a motor vehicle collision, the presence of an isolated seatbelt sign was not associated with any cases of cerebrovascular injury. [5]
Management
- Prehospital
- Hospital
- Secure ABCs
- See specific diagnosis
Disposition
- Based on specific diagnosis
See Also
- Penetrating neck trauma
- Cervical spine clearance
- Canadian cervical spine rule
- NEXUS cervical spine rule
References
- ↑ 27. Hoffman JR, et al. Low-risk criteria for cervical-spine radiography in blunt trauma: a prospective study. Ann Emerg Med 1992;21:1454-60.
- ↑ Mahadevan, et al. Interrater reliability of cervical spine injury criteria inpatients with blunt trauma. Ann Emerg Med1998;31:197-201
- ↑ DiPerna CA, Rowe VL, Terramani TT, et al. Clinical importance of the “seat belt sign” in blunt trauma to the neck. Am Surg. 2002;68:441–445
- ↑ Rozycki GS, Tremblay L, Feliciano DV, et al. A prospective study for the detection of vascular injury in adult and pediatric patients with cervicothoracic seat belt signs. J Trauma. 2002;52:618–623; discussion 623–624
- ↑ Desai NK, et al. Screening CT angiography for pediatric blunt cerebrovascular injury with emphasis on the cervical “seat- belt sign.” AJNR Am J Neuroradiol. 2014 Sep;35(9):1836-40. PMID: 24722311.