We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Retroperitoneal hemorrhage
From WikEM
Contents
Background
- Bleeding into retroperitoneal space
- Difficult to diagnose given poor sensitivity of physical exam findings (Cullens, Grey-Turners)
- Can accumulate 4L blood before tamponade
Etiologies
- Trauma (renal, vascular, colon, pancreas or pelvis)
- Leaking/ruptured AAA
- Iatrogenic (colonoscopy, cardiac catheterization, femoral line placement)
- Spontaneous (coagulopathy)
- Hemorrhagic pancreatitis
Clinical Features
- Most common in patients with bleeding disorders, on anticoagulants, and on HD[1][2]
- May present with:
- Abdominal pain
- Flank pain
- Back pain
- Hypotension
- Bryant's sign (unilateral scrotal ecchymosis from tracking blood)
Differential Diagnosis
Abdominal Trauma
- Liver trauma
- Splenic trauma
- Pelvic fractures
- Genitourinary trauma
- Retroperitoneal hemorrhage
- Renal trauma
- Ureter trauma
- Abdominal compartment syndrome
- Trauma in pregnancy
Evaluation
Must have high clinical suspicion to make diagnosis
- CT scan abdomen/pelvis
- Consider ultrasound for AAA
- FAST and DPL do not evaluate retroperitoneal space
Classification of traumatic retroperitoneal hemorrhage
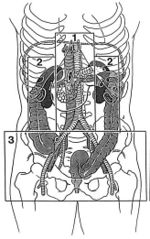
- Zone 1: Central[3]
- Pancreaticoduodenal injuries, major vascular injury
- Zone 2: Flank/Perinephric
- Renal trauma, ureteric or colonic injury
- Zone 3: Pelvic
- Pelvic fracture or ileofemoral vascular injury
Management
- Address A, B, C's
- Resuscitation with blood products
- Reverse coagulopathy
- Treat underlying etiology
Disposition
- ICU
See Also
- Abdominal trauma
- coagulopathy
- Warfarin (Coumadin) Reversal
- Dabigatran (Pradaxa) Reversal
- Unfractionated heparin reversal
- Aortic ultrasound
External Links
References
- ↑ Bhasin HK and Dana CL. Spontaneous retroperitoneal hemorrhage in chronically hemodialyzed patients. Nephron. 1978; 22(4-6):322-327.
- ↑ Ernits M, et al. A retroperitoneal bleed induced by enoxaparin therapy. Ann Surg. 2005; 71(5):430-433.
- ↑ FELICIANO, D. V. (1990) ‘Management of Traumatic Retroperitoneal Hematoma’, Annals of Surgery, 211(2), pp. 109–123.
Authors
Kenn Ghaffarian, Neil Young, Kian Preston-Suni, Ross Donaldson