We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Wellens' syndrome
From WikEM
Contents
Background
Initially described in 1982 where a subset of patients who did poorly with medical management of “impending myocardial infarction” (essentialy unstable angina) were found to have characteristic ECG changes. These patients were noted to be at increased risk for extensive anterior wall myocardial infarctions due to proximal LAD stenosis.[1]
- T wave abnormality that is associated with critical LAD stenosis[2]
- Finding can be transient (persists for hours after pain has resolved and then disappears)
- Preinfarction stage of CAD
- Natural history may include progression to extensive anterior wall myocardial infarction, often associated with severe left ventricular systolic dysfunction, cardiogenic shock and even death
Clinical Features
Refer to Myocardial infarction
- May be pain free at presentation and time of ECG
- May have had previous recent episode of angina +/- associated symptoms
- Initial cardiac enzymes are frequently normal or only slightly elevated[3][4]
- Cocaine may cause pseudo-Wellens due to vasospasm without critical stenosis[5]
Differential Diagnosis
- High voltage
- PE
- RBBB
- Hypokalemia
- CNS Injury
- Persistent Juvenile T-wave pattern
- Digitalis Effect
- "Normal variant" STE with biphasic T-wave[6]
- Common in young, healthy, Black males
- Patterns that are NOT found in Wellen's
- High voltage complexes
- Notching at J-point ("fishhook")
- Concave upward ST segment followed by steep drop in T wave
ST Elevation
- Myocardial infarct (STEMI)
- Post-MI (ventricular aneurysm pattern)
- Previous MI with recurrent ischemia in same area
- Wellens' syndrome
- Coronary artery vasospasm (eg, Prinzmetal's angina)
- Coronary artery dissection
- Drugs of abuse (eg, cocaine, crack, meth)
- Pericarditis
- Myocarditis
- Aortic dissection in to coronary
- LV aneurysm
- Early repolarization
- Left bundle branch block
- Left ventricular hypertrophy (LVH)
- Pneumomediastinum
- Pneumothorax
- Pulmonary Embolism
- Myocardial tumor
- Myocardial trauma
- External compression of artery
- Medications: Tricyclic (TCA) toxicity, Digoxin
- RV pacing (appears as Left bundle branch block)
- Hyperkalemia (only leads V1 and V2)
- Hypothermia ("Osborn J waves")
- Brugada syndrome
- Takotsubo cardiomyopathy
- AVR ST elevation
Evaluation
- History of chest pain
- Normal or slightly-elevated cardiac enzymes
- No precordial Q-waves
- Isoelectric or <1mm ST-segment elevation
- Pattern present in pain-free state
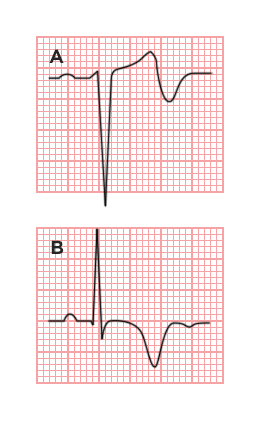
Two T-wave Characteristics (at times terms are reversed in the literature or labeled Type I and II):
- Type A (25%): Biphasic T-wave in V2/V3
- Type B (75%): Deep, symmetrically inverted T-waves in V2/V3
Note Wellens criteria should not be diagnosed in a patetient with LVH.;
Management
- Urgent cardiac catheterization
- Stress testing contraindicated
See Also
External Links
Mattu ECG Case - Wellens' Syndrome
Video
References
- ↑ de Zwaan C, Bär FW, Wellens HJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982;103(4 Pt 2):730-736.
- ↑ Rhinehardt J, Brady WJ, Perron AD, Mattu A. Electrocardiographic manifestations of Wellens' syndrome. American Journal of Emergency Medicine. 2002;20(7):638-643. doi:10.1053/ajem.2002.34800.
- ↑ Ünlüer EE et al. Red Flags in Electrocardiogram for Emergency Physicians: Remembering Wellens' Syndrome and Upright T wave in V1. West J Emerg Med. 2012 May; 13(2): 160–162.
- ↑ Kannan L and Figueredo VM. Wellens' Syndrome. Jan 1, 2015. N Engl J Med 372;1.
- ↑ Dhawan SS. Pseudo-Wellens’ syndrome after crack cocaine use. Can J Cardiol. 2008; 24(5):404.
- ↑ Wang, et al. ST-segment elevation in conditions other than acute myocardial infarction. NEJM 2003, 349:2128-2135.