

FoodNet Surveillance
 ShareCompartir
ShareCompartir
Active Laboratory Surveillance
FoodNet has conducted population-based surveillance for laboratory-confirmed cases of infection caused by Campylobacter, Listeria, Salmonella, Shiga toxin-producing Escherichia coli (STEC) O157, Shigella, Vibrio, and Yersinia since 1996; Cryptosporidium and Cyclospora since 1997; and STEC non-O157 since 2000. In 2009, FoodNet began to collect information on STEC and Campylobacter cases that were identified by culture-independent methods and expanded this to Listeria, Salmonella, Shigella, Yersinia, and Vibrio in 2011.
FoodNet is an active surveillance system, meaning that public health officials routinely communicate with more than 650 clinical laboratories serving the surveillance area to identify new cases and conduct periodic audits to ensure that all cases are reported.
FoodNet collects information on laboratory-confirmed cases (defined as isolation for bacteria or identification for parasites of an organism from a clinical specimen) and cases diagnosed using culture-independent methods. Once a case is identified, FoodNet personnel at each site collect information about core variables and enter this information into a database, and transmit data to CDC. The data include:
- Hospitalizations occurring within 7 days of the specimen collection date,
- The patient’s status (alive or dead) at hospital discharge (or at 7 days after the specimen collection date if the patient is not hospitalized),
- Whether the patient traveled abroad in the 7 days before illness began, and selected food and environmental exposures for select pathogens.
FoodNet also conducts surveillance for cases of hemolytic uremic syndrome (HUS) through a network of pediatric nephrologists and infection-control practitioners who report all illnesses diagnosed as HUS on the basis of physician diagnosis. FoodNet staff review hospital discharge data for pediatric HUS cases to validate surveillance reports and identify additional cases by using ICD-9-CM/ICD-10 codes specifying HUS, acute renal failure with the hemolytic anemia and thrombocytopenia, or thrombotic thrombocytopenic purpura with diarrhea caused by an unknown pathogen or E. coli.
In addition to routine surveillance, FoodNet also conducts special surveillance projects. In 2002, two sites conducted population-based surveillance for reactive arthritis associated with Campylobacter, Salmonella, Shigella, Yersinia, and STEC infections. In 2009, FoodNet conducted a pilot surveillance program for community-acquired Clostridium difficile infections in Connecticut and New York. In 2010, FoodNet conducted a pilot surveillance program for Cronobacter sakazakii infections in selected sites.
Burden of Illness
The burden of illness pyramid is a model for understanding foodborne disease reporting , and illustrates steps that must occur for an episode of illness in the population to be registered in surveillance.
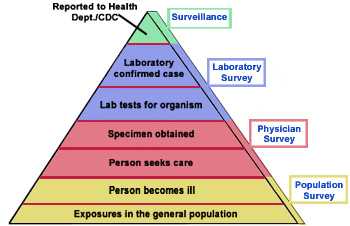
The burden of illness pyramid is a model for understanding foodborne disease reporting.
Starting from the bottom of the pyramid:
- Some members of the general population are exposed to an organism;
- Some of these exposed people become ill;
- Some of these ill people seek medical care;
- A specimen is obtained from some of these people and submitted to a clinical laboratory;
- A laboratory tests some of these specimens for a given pathogen;
- The laboratory identifies the causative organism in some of these tested specimens and thereby confirms the case;
- The laboratory-confirmed case is reported to a local or state health department.
FoodNet conducts laboratory surveys, physician surveys, and population surveys to collect information about each of these steps. This information is used to calculate estimates of the actual number of people who become ill. Other information is used to estimate the proportion of these illnesses transmitted by food.
- Page last reviewed: May 14, 2015
- Page last updated: December 7, 2015
- Content source: