We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Febrile seizure
From WikEM
Contents
Background
- 50% of patients never have temperature >39
- Antipyretics do not offer significant improvements in recurrence rates of febrile seizures[1]
- Febrile seizures do not increase the risk of serious bacterial illness
Prognosis
- 2-3% chance of developing epilepsy (1% for general population)
- 50% of patients <12 mo will have another simple febrile seizure
- 30% of patients >12 mo will have another simple febrile seizure
Clinical Features
Differential Diagnosis
Pediatric seizure
- Seizure
- Febrile seizure
- First-Time afebrile seizure
- Neonatal seizure
- Epileptic seizures
- Seizure with VP shunt
- Impact seizure (trauma)
- Status epilepticus
- Meningitis
- Intracranial mass
- Epidural/subdural infection or hematoma
- Toxic ingestion
- Hydrocephalus
- Pyridoxine responsive seizure[2]
Pediatric fever
- Upper respiratory infection (URI)
- UTI
- Sepsis
- Meningitis
- Febrile seizure
- Pneumonia
- Acute otitis media
- Whooping cough
- Unclear source
- Kawasaki disease
- Neonatal HSV
Evaluation
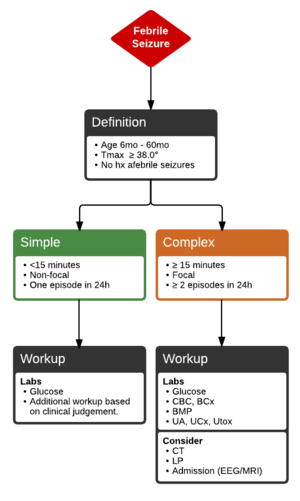
Simple versus Complex
- Simple
- Generalized tonic-clonic seizure
- <15 min in duration
- Age 6mo - 5yr
- Occurs only once in 24hr period
- No focal features
- Complex
- Any exception to above
Work-Up
- Glucose in all patients
Simple febrile seizure
- Neither labs nor neuroimaging are absolutely necessary
- Normal pediatric fever workup
Complex febrile seizure
- Consider CBC, blood culture, UA, urine culture, CSF studies
- Consider CT if:
- Persistently abnormal neuro exam (especially with focality)
- Signs/symptoms of increased ICP
- Patient has VP shunt
- Consider ECG if:
- Routine EEG not indicated
- Consider only if developmental delay or for focal symptoms
- Causes amenable to specific treatment
- Hypoglycemia
- Hyponatremia (water intoxication, dilution of formula)
- Hypocalcemia
- Hypomagnesemia
- INH ingestion
Management
Ongoing Seizure
See Seizure (peds)
Seizure Stopped
- Treat underlying infection if indicated
Disposition
Discharge
- Simple febrile seizure if patient at baseline
- Follow-up in 1-2d
- Complex febrile seizure if patient well-appearing, work-up normal
- Follow-up in 24hr
Admit
- Ill-appearing
- Lethargy beyond postictal period
See Also
References
- ↑ Rosenbloom E, et al. Do antipyretics prevent the recurrence of febrile seizures in children? A systemic review of randomized controlled trials and meta-analysis. Eur J Paediatr Neurol. 2013; 17:585-588.
- ↑ Baxter P. et al. Pyridoxine‐dependent and pyridoxine‐responsive seizures. Developmental Medicine & Child Neurology 2001, 43: 416–42