We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Posterior shoulder dislocation
From WikEM
Contents
Background
- Accounts for 2-4% of shoulder dislocations[1]
- Mechanism of injury - forceful internal rotation/adduction (secondary to e.g. seizure, electric shock) or blow to ant shoulder
- Neurovascular and rotator cuff tears are less common than in ant dislocations
Clinical Features
- Prominence of posterior shoulder and ant flattening of normal shoulder contour
- Patient unable to rotate or abduct affected arm
Differential Diagnosis
Shoulder and Upper Arm Diagnoses
Traumatic/Acute:
- Shoulder Dislocation
- Anterior shoulder dislocation
- Posterior shoulder dislocation
- Inferior shoulder dislocation
- Clavicle fracture
- Humerus fracture
- Scapula fracture
- Acromioclavicular injury
- Glenohumeral instability
- Rotator cuff tear
- Biceps tendon rupture
- Triceps tendon rupture
- Septic joint
Nontraumatic/Chronic:
- Rotator cuff tear
- Impingement syndrome
- Calcific tendinitis
- Adhesive capsulitis
- Biceps tendinitis
- Subacromial bursitis
Refered pain & non-orthopedic causes:
- Referred pain from
- Neck
- Diaphragm (e.g. gallbladder disease)
- Brachial plexus injury
- Axillary artery thrombosis
- Thoracic outlet syndrome
- Subclavian steal syndrome
- Pancoast tumor
- Myocardial infarction
- Pneumonia
- Pulmonary embolism
Evaluation
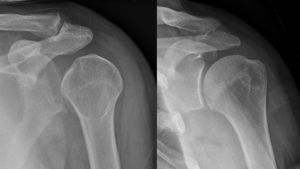
- Plain film X-ray
- Scapular "Y" view shows humeral head in posterior position
- Lack of normal overlap of humeral head and glenoid fossa
- "Light bulb sign" - fixed internal rotation makes for light bulb appearance of humeral head on AP
- Bedside ultrasound can be used to assess for both dislocation and successful reduction
Management
- Reduce
- Consider procedural sedation
- Traction applied to adducted arm in long axis of humerus
- Assistant pushes humeral head anteriorly into glenoid fossa
- Post-reduction X-ray
- Apply sling
Disposition
- Discharge after reduction
- Ortho follow-up
See Also
External Links
References
- ↑ Grate I Jr. Luxatio erecta: a rarely seen, but often missed shoulder dislocation. Am J Emerg Med. 2000 May;18(3):317-21.