We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Shoulder dislocation
From WikEM
Contents
Background
- Humerus separates from the scapula at the glenohumeral joint
- Partial dislocation of the shoulder is referred to as subluxation
Types
Differential Diagnosis
Shoulder and Upper Arm Diagnoses
Traumatic/Acute:
- Shoulder Dislocation
- Clavicle fracture
- Humerus fracture
- Scapula fracture
- Acromioclavicular injury
- Glenohumeral instability
- Rotator cuff tear
- Biceps tendon rupture
- Triceps tendon rupture
- Septic joint
Nontraumatic/Chronic:
- Rotator cuff tear
- Impingement syndrome
- Calcific tendinitis
- Adhesive capsulitis
- Biceps tendinitis
- Subacromial bursitis
Refered pain & non-orthopedic causes:
- Referred pain from
- Neck
- Diaphragm (e.g. gallbladder disease)
- Brachial plexus injury
- Axillary artery thrombosis
- Thoracic outlet syndrome
- Subclavian steal syndrome
- Pancoast tumor
- Myocardial infarction
- Pneumonia
- Pulmonary embolism
Evaluation
- Plain film X-ray
- Ultrasound

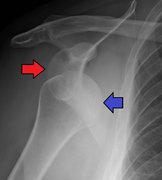
Anterior shoulder dislocation on Y-view

Anterior shoulder dislocation with fracture


Management
- Reduction
- See individual types for specific techniques
- Cochrane review notes lower complications, equal pain control, and shorter ED stay with intra-articular lidocaine vs. procedural sedation
- 20 mL of 1% lidocaine intra-articular injection[1]
Disposition
- Uncomplicated dislocation can be discharged after reduction
- Recurrence rate around 27% if older than 30 years and 72% is younger than 23 years[2]
See Also
External Links
Video
References
- ↑ Intra-articular lignocaine versus intravenous analgesia with or without sedation for manual reduction of acute anterior shoulder dislocation in adults (Review) Cochrane Database Syst Rev. 2011 Apr 13;(4):CD004919 full text
- ↑ Watson S, Allen B, Grant JA. A Clinical Review of Return-to-Play Considerations After Anterior Shoulder Dislocation. Sports Health. 2016; 8(4):336-341.