


Behavioral Risk Factor Surveillance System
 ShareCompartir
ShareCompartir
Monitoring Health Risks and Behaviors Among Adults
At A Glance 2016
The Behavioral Risk Factor Surveillance System (BRFSS) is the nation’s premier system of telephone surveys that collect state data about health risk behaviors, chronic health conditions, and use of preventive services among US residents.
For more than 30 years, the Centers for Disease Control and Prevention (CDC), all 50 states, the District of Columbia (DC), and participating US territories have used the BRFSS to collect uniform, state-specific information about a wide range of behaviors that affect the health of US adults.
Public Health Problem
States Need Data to Improve Population Health
For most states, the BRFSS is the only source of state data on health and health risk behavior related to chronic disease. The BRFSS gives communities and states, as well as CDC and other federal agencies, the information they need to plan, conduct, and evaluate public health programs and other activities at local, state, and national levels.
With more than 450,000 adults interviewed each year across the United States and participating territories, the BRFSS is the largest continuous telephone health surveillance system in the world. Each year, states can choose to add several optional modules to their core surveys. These modules are sets of questions about various health topics, such as the respondents’ experiences with chronic illnesses, workplace conditions, diet, and prevention behaviors like disease screenings and immunizations. States can also add questions that they develop to meet their specific needs.
All states use the same methods to conduct their surveys, as well as any additional modules and state-added questions. This consistency produces results that public health professionals can compare between states or local areas.
To see how BRFSS data are used by public health experts and policy makers in all 50 states, DC, and US territories, visit the BRFSS website.
CDC Works to Ensure Quality Data
CDC works to ensure the success of the BRFSS by giving states the support they need to administer their questions and analyze their data correctly and consistently. To ensure high-quality BRFSS data, CDC processes survey data, produces monthly and annual data quality reports, and provides training for state BRFSS coordinators and their staff. CDC also helps states develop their capacity to analyze, interpret, and use their survey data.
In 2011, CDC added a cell phone survey to improve the reach of the BRFSS. A new method for weighting BRFSS data allows for the inclusion of cell phone data and increases the validity of estimates. BRFSS staff are also working to keep telephone interviews to a reasonable length, while still allowing states to add questions to meet changing needs.
CDC’s Response
The National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP) works in four key areas or domains: epidemiology and surveillance, environmental approaches, health care system interventions, and community programs linked to clinical services. This comprehensive approach supports healthy choices and behaviors, makes healthier options more available, and helps Americans better manage their health.
CDC works with state and territorial partners to collect data about health and wellness that can be used to make decisions about public health research, practice, and policies. With about $18 million in FY 2015 funding, the BRFSS supports these efforts by focusing its activities in one of NCCDPHP’s four domains: epidemiology and surveillance.
Related Materials

Fast Facts
- More than 450,000 US adults are interviewed as part of the BRFSS each year.
- In 2014, states collected 36% of BRFSS data by cell phone.
- All states use a standard core questionnaire, and they can add their own questions. The BRFSS also provides standard optional modules on about 30 additional topics.
- Core questions and optional modules collect information about health risk behaviors related to nutrition, physical activity, tobacco and alcohol use, diabetes, heart disease, immunizations, injuries, health care access, and use of health care services.

Percentage of US Adults Who Reported Fair or Poor Health, 2014
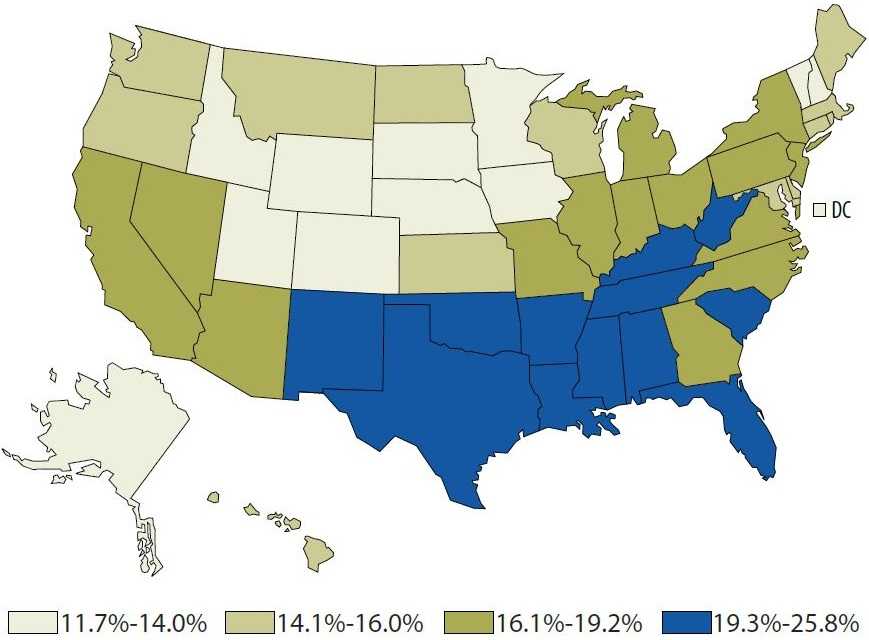
Data source: Behavioral Risk Factor Surveillance System.
Complete data points are also available.
Epidemiology and Surveillance
Collecting Asthma Data to Improve Programs
Since 2005, BRFSS respondents who report a diagnosis of asthma have been asked to participate in a follow-up Asthma Call-Back Survey (ACBS). Results from the ACBS in Mississippi showed that asthma rates in the state were high, particularly among minority populations and children. The BRFSS is helping state leaders address this public health problem by providing reliable prevalence rates by residents’ gender, race, socioeconomic status (education and income), and county.
The ACBS data are also being used in Mississippi to train caregivers, health care workers, and asthma educators; tailor interventions to residents at highest risk; and help state leaders make informed policy decisions. For example, these data were used to support a comprehensive state law that allows students to carry and use asthma medications on school grounds.
Mississippi Residents with Current Asthma, 2014
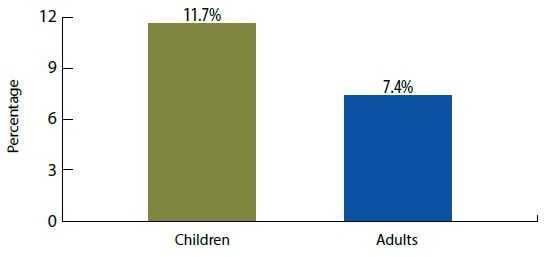
Data source: Behavioral Risk Factor Surveillance System.
Using Workplace Data to Identify Health Risks
In Massachusetts, state health officials and CDC’s National Institute for Occupational Safety and Health (NIOSH) used BRFSS data to identify the level of secondhand smoke exposure in state workplaces. Researchers found a decline in smoking and secondhand smoke exposure among nonsmokers after a smoke-free workplace law was passed in the state. However, the data suggested that workers in some occupations (e.g., construction, maintenance, transportation, installation) were not benefitting as much as others. State officials are looking for other ways to protect these workers, such as by encouraging the expansion of smoke-free housing policies.
Other states have also worked with NIOSH to conduct studies with BRFSS work-related data. Examples include examinations of health-related habits among health care workers in New Hampshire and the association between obesity rates and occupation in Washington.
Tracking Health Data on Mothers and Babies
In 2007, state officials in North Carolina created the North Carolina Preconception Health Coalition. They used BRFSS data to develop the coalition’s strategy and write the North Carolina Preconception Health Strategic Plan. They also worked with stakeholders to use BRFSS data to design educational materials, develop a social marketing strategy, and support program development.
Members of the leadership team continue to use BRFSS data to track the state’s progress on preconception health and to assess the effectiveness of state initiatives.
States and territories collect BRFSS data through telephone interviews with noninstitutionalized adults aged 18 or older. Interviewers call potential participants on both landlines and cell phones.
The resulting data sets provide details about respondents’ health and health-related behaviors, as well as selected demographic information. CDC posts these data sets on the BRFSS website for public use.
BRFSS data help public health practitioners and researchers work to improve population health by
- Identifying and addressing health risks and vulnerable populations.
- Monitoring changes in health risk behaviors and diseases.
- Evaluating public health programs.
- Establishing prevention strategies at local and state levels.

“The BRFSS is currently the only source of population-based estimates of the prevalence of various health behaviors, medical conditions, and preventive health care practices among Michigan adults. BRFSS findings are critical to state-based public health agencies, academic institutions, and nonprofit organizations in their development of programs that promote the health of Michigan citizens.”
Chris Fussman, MS
BRFSS Coordinator
Michigan Department of Health and Human Services
Training Health Department Staff
CDC provides training opportunities to hundreds of health department staff and other public health practitioners and researchers working at state, territorial, and local levels in the United States and across the world. These trainings include a conference held every other year that is also well-attended by academics and students of public health.
Conference attendees have come from as far away as the Federated States of Micronesia, Bangladesh, Brazil, Scotland, and Thailand to learn from BRFSS experts. In 2013, a group from Colombia attended to learn about sampling options for a risk factor surveillance system being developed in their country.
The BRFSS conference features trainings in “tools of the trade” skills like survey design, weighting, statistics, use of analytic software and computer-aided data collection technology, research techniques using BRFSS data sets, and small-area estimation. It also includes scientific presentations and poster sessions on dozens of BRFSS-related studies on a range of topics, from health care problems among Native Alaskans to public health surveillance in Guam.
The conference also gives state BRFSS coordinators a chance to learn from their colleagues’ experiences with data collection and analysis, talk about public health surveillance needs, and discuss the next year’s BRFSS survey.
Future Directions
CDC will continue to work with state and federal partners to collect high-quality data that can be used to help states set and track health objectives, plan health programs, conduct disease prevention and health promotion activities, and monitor trends. Ongoing challenges include getting people to participate in BRFSS surveys and adapting to changes in communications technology and population diversity.
The BRFSS also continues to expand its use of local data. For example, for the past decade, the BRFSS has provided local health information about several metropolitan and micropolitan areas through the Selected Metropolitan/Micropolitan Area Risk Trends (SMART) project.
In 2016, CDC will begin posting county data on health indicators through the BRFSS Small-Area Estimates (SAE) project. Information will be available initially for selected chronic diseases (e.g., asthma, diabetes, heart disease), health care access, and health-related behaviors (e.g., physical activity, alcohol and tobacco use). Additional indicators will be added over time.

The BRFSS has been successful because it shares ownership of the data collected with its local partners, according to David McQueen, ScD, keynote speaker for the 2013 BRFSS conference.
- Page last reviewed: January 26, 2016
- Page last updated: January 26, 2016
- Content source: