


Infant Health
 ShareCompartir
ShareCompartir
Protecting Our Next Generation
At A Glance 2016
Becoming a parent is one of life’s greatest joys. By improving health before pregnancy, we can prevent many future problems for mothers and babies. The Centers for Disease Control and Prevention (CDC) is at the forefront of the nation’s efforts to promote health and prevent and control chronic diseases so that all women can have a safe and healthy pregnancy.
The ideal result is a full-term pregnancy without unnecessary interventions, the delivery of a healthy baby, and a healthy postpartum period in a positive environment that supports the physical and emotional needs of the mother, baby, and family. Families are encouraged to trust their instincts and to meet with their health care providers early. The earlier problems are detected, the sooner prevention and life-saving treatment can begin.
Public Health Problem
Infant Mortality
In 2014, there were almost 4 million live births in the United States. Although most newborns grow and thrive, more than 23,000 infants died in 2014. For every 1,000 infants born, 6 die before their first birthday. The US infant death rate has declined 13% since 2005, but is still twice as high for black infants than for white infants.
The five leading causes of infant death are birth defects, preterm birth or low birth weight, maternal complications of pregnancy, sudden infant death syndrome (SIDS), and unintentional injuries.
Preterm Birth
Although preterm births (before 37 weeks of pregnancy) have declined 8% since 2007, nearly 1 in 10 infants (about 380,000) were born prematurely in 2014. The earlier an infant is born, the more likely he or she is to require intensive and prolonged hospitalization and have higher medical costs. Premature infants are also more likely to have lifelong health problems, such as cerebral palsy, developmental delays, chronic lung disease, and vision and feeding problems. Infant death rates related to preterm birth are three times higher for black infants than for white infants.
Assisted Reproductive Technology (ART) Challenges
ART helps many couples overcome problems with infertility. However, women who conceive through ART are at higher risk of preterm birth and low birth weight infants, mainly because they have a greater chance of becoming pregnant with two or more infants at a time. Carrying and delivering two or more infants at a time is associated with a higher risk of complications for both women and infants.
Sudden Unexpected Infant Death (SUID) and SIDS
About 3,500 infants died suddenly and unexpectedly before their first birthday in 2014. Although the cause of death cannot always be explained, most deaths occurred while the infant was sleeping in an unsafe environment. Researchers do not know how often these deaths are caused by accidental suffocation from soft bedding or from another person rolling on top of or against the infant while sleeping. Often, no one witnesses these deaths, and no tests exist to tell SIDS from suffocation. Most SUID cases are reported as SIDS, unknown causes, or accidental suffocation and strangulation in bed.
Related Materials

Fast Facts
- In 2014, there were almost 4 million live births in the United States.
- The US infant death rate has declined by 13% since 2005, its most recent peak.
- Despite declines, the death rate is still two times higher for black infants than for white infants.
- Preterm births (less than 37 weeks) have declined by 8% since 2007.
- CDC is working with partners to prevent infant deaths by addressing the risk factors that affect birth outcomes.

Infant Death Rates, by Race and Hispanic Origin, United States, 2014
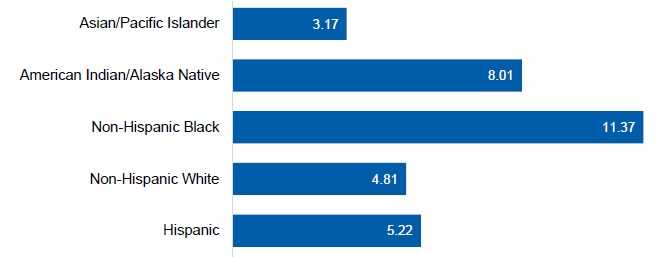
Rate per 1,000 Live Births
Note: Infant death is defined as death before the first birthday.
Source: National birth and death files acessed through CDC WONDER.
CDC’s Response
The National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP) works in four key areas or domains: epidemiology and surveillance, environmental approaches, health care system interventions, and community programs linked to clinical services. This comprehensive approach supports healthy choices and behaviors, makes healthier options more available, and helps Americans better manage their health.
CDC works with partners—such as public health agencies, other federal agencies, academia, and community organizations—to improve the health of women before, during, and after pregnancy. The agency is committed to reducing infant deaths by addressing the social, behavioral, and health risk factors that affect birth outcomes.
With $46 million in FY 2016 funding, CDC’s Division of Reproductive Health supports these efforts by focusing its activities in two of NCCDPHP’s four domains: epidemiology and surveillance and health care system interventions.
Epidemiology and Surveillance
Improving SUID Reporting
CDC conducts population-based surveillance at 18 grantee sites, covering 30% of all SUID cases in the United States. A better understanding of the circumstances and events associated with SUID and sleep-related infant deaths may help reduce future deaths. CDC’s activities related to SUID and SIDS are designed to standardize and improve data collected at infant death scenes and to promote consistent reporting and classification of SUID cases. Examples of CDC’s efforts in this area include the following:
SUID Case Registry: CDC funds 16 states and 2 jurisdictions to compile comprehensive information about the circumstances associated with SUID cases, as well as information about investigations into these deaths. Grantees use SUID data to monitor trends, plan and evaluate SUID prevention programs, modify public health practice and policy for state maternal and child health programs, and encourage more consistent medical and legal practices.
Sudden Death in the Young (SDY) Case Registry: CDC and the National Institutes of Health collaborate on this surveillance system, which compiles comprehensive information on sudden unexpected cardiac and neurologic deaths among infants, children, and adolescents. Currently, 10 states or jurisdictions participate in the SDY Case Registry.
National ART Surveillance System (NASS)
NASS tracks ART use and outcomes across the United States. CDC uses this system to collect data from more than 460 fertility clinics, calculate standardized success rates for each clinic, and publish the results in the annual Assisted Reproductive Technology Fertility Clinic Success Rates Report. This report gives consumers information about national and clinic-specific ART success rates. NASS also allows researchers to assess infant outcomes (e.g., birth weight, plurality, maturity) and monitor trends in ART use.
Over the last decade, ART use in the United States has doubled. According to preliminary NASS data, 208,786 ART cycles were performed at 460 reporting clinics in 2014, resulting in the live birth of 70,352 infants.
Maternal and Child Health Epidemiology Program (MCHEP)
MCHEP assigns senior CDC epidemiologists and graduate-level fellows to state health departments and other public health agencies and organizations. These embedded staff help states build their epidemiologic infrastructure and provide direct assistance on a variety of topics, including infant health and preterm birth. In 2016, a total of 13 senior MCH epidemiologists and 11 fellows from the Council of State and Territorial Epidemiologists are working in 15 public health agencies or organizations. They are helping states develop programs and policies to improve the health and well-being of women, infants, children, and families.
“Advanced medical technology and effective public health strategies have drastically reduced the number of babies born too early and dying too early in our country, but we still have more work to do. By promoting prevention strategies that we know are effective, we can give the next generation a healthier future.”
Wanda D. Barfield, MD, MPH
Director of CDC’s Division of Reproductive Health
Pregnancy Risk Assessment Monitoring System (PRAMS)
PRAMS collects state-specific population data on maternal attitudes, experiences, and health before, during, and shortly after delivery. CDC uses PRAMS to identify women and infants at risk of health problems, monitor access to care and services, identify changes in behavior and health status, and measure progress in improving the health of mothers and infants. In FY 2016, 40 states and New York City are participating, representing about 78% of all live births in the United States. In FY 2017, PRAMS plans to expand to all 50 states and Puerto Rico.
State governments use PRAMS data to develop and review programs and policies to reduce health problems among mothers and infants. For example:
- Maryland used PRAMS data to support legislation on a statewide ban on the sale of crib bumpers, which have been linked to SIDS.
- In Florida, the data were used to support efforts that led to Florida Medicaid covering flu shots for pregnant enrollees.
- North Carolina used the data to support an educational and social marketing campaign that promotes breastfeeding.

Health Care System Interventions
In 2011, CDC funded state perinatal quality collaboratives (PQCs) in California, New York, and Ohio to continue and enhance their work promoting quality perinatal care statewide, with an emphasis on reducing elective deliveries before 39 weeks’ gestation. In 2014, CDC added three new states—Illinois, Massachusetts, and North Carolina.
Funding from CDC will enhance the ability of the PQCs to improve the quality of perinatal care in their states, including efforts to:
- Reduce maternal complications associated with high blood pressure.
- Improve care for infants with complications due to maternal substance abuse.
- Improve the use of progesterone drugs to reduce preterm birth.
- Improve the accuracy and timeliness of birth certificate data.
In partnership with the PQCs, CDC hosts regular webinars that allow states to share information about their program development strategies and quality improvement initiatives.
The PQCs’ efforts have helped to reduce early elective deliveries in the United States. For example, in Ohio, the births of about 48,400 infants that would have been delivered at 37 to 39 weeks were appropriately delayed to 39 weeks or more during 2008-2015. As a result, more than $27 million in health care costs were saved because these infants did not need neonatal intensive care. Nationwide, early elective deliveries have decreased, reaching the target rate of less than 5% in 2013 and 2014.
Future Directions
CDC will continue to work to reduce the infant death rate and help address the social, behavioral, and health risk factors that affect birth outcomes. Priority areas include the following:
- Reducing preterm delivery and racial and ethnic disparities.
- Reducing elective deliveries before 39 weeks.
- Increasing the number of preterm infants that get life-saving care at neonatal intensive care units.
- Conducting surveillance of risks, behaviors, and knowledge among pregnant women to improve preconception, maternal, and infant health.
- Standardizing and improving data collected at infant death scenes and promoting consistent reporting and classification of SUID cases.
- Understanding the relationship between ART and preterm birth.
- Page last reviewed: May 26, 2016
- Page last updated: May 26, 2016
- Content source: