


Maternal Health
 ShareCompartir
ShareCompartir
Advancing the Health of Mothers in the 21st Century
At A Glance 2016
Maternal health has significantly improved in the 21st century, but too many women continue to die or suffer severe pregnancy complications every year. An increasing number of pregnant women in the United States have chronic conditions such as high blood pressure, diabetes, or heart disease that may put them at risk of pregnancy complications or death.
The Centers for Disease Control and Prevention (CDC) is committed to conducting research and supporting efforts that will help women have safe and healthy pregnancies.
Public Health Problem
Pregnancy-Related Deaths
Despite advances in medicine and medical technologies, the rate of pregnancy-related deaths in the United States has increased over the past 25 years. However, recent data show that this trend may be leveling off.
One in four pregnancy-related deaths are related to heart conditions. Women also die of infections (including flu), bleeding, blood clots, and high blood pressure. Although the risk of dying of pregnancy complications is low, some women are at higher risk than others.
- African American women are 3 to 4 times more likely to die of pregnancy complications than white women.
- Women aged 35 to 39 are almost twice as likely to die of pregnancy complications as women aged 20 to 24. The risk becomes even higher for women aged 40 or older.
Severe Maternal Morbidity
The most severe pregnancy complications, such as a heart attack or hemorrhage, are also known as severe maternal morbidity (SMM). Every year, SMM affects about 65,000 women in the United States, and this number is increasing.
The rate of SMM more than doubled from 2000 to 2010, leading to higher direct medical costs and extended hospital stays. This increase could be driven by a combination of factors, such as increases in maternal age, prepregnancy obesity, preexisting chronic conditions, and cesarean or other complications during delivery. Tracking SMM cases is one way to identify priority areas for interventions in maternal care, focus quality improvement where it will make the most difference, and determine if these interventions are effective.
Chronic Conditions and Risk Behaviors
A woman’s weight before pregnancy and weight gain during pregnancy are important indicators of the current and future health of both mother and child. Recent CDC studies showed that nearly half of women are overweight or obese before they become pregnant, which is associated with a higher risk of pregnancy complications. Gaining more weight than recommended during pregnancy can result in a baby born at an unhealthy weight and can make it harder for the mother to lose excess weight after delivery. This excess pregnancy weight gain may lead to future obesity for both mother and child. A CDC study showed that, in 2013, nearly half of women gained too much weight during pregnancy.
Maternal smoking is also an ongoing public health problem in the United States. In addition to the well-known health risks for the baby (e.g., preterm birth, sudden infant death syndrome), smoking during pregnancy increases the risk of complications for the mother. These complications can range from problems with the placenta to her water breaking early.
In 2013, about 1 in 5 women smoked in the 3 months before pregnancy, and about 1 in 10 smoked during the last 3 months of pregnancy, according to Pregnancy Risk Assessment Monitoring System (PRAMS) data from 27 states. In addition, about 5% of women used illegal drugs during pregnancy.
Mental health disorders such as depression are also common and can affect the health and well-being of women and their families. About 1 in 9 pregnant women had symptoms of major depression in 2013. However, only about half of pregnant women with depression received treatment for this condition.
Preconception Health
A healthy pregnancy begins long before a woman conceives. Preconception health refers to things women can do before and between pregnancies to increase the chance of having a healthy baby and being a healthy mother. All women of reproductive age should try to adopt a healthy lifestyle and address any health problems. Women should also visit their health care provider if they are thinking about getting pregnant to ensure that they receive the correct medical advice. At every medical visit with women of reproductive age, health care providers should discuss reproductive plans, prescribe contraception if appropriate, and address chronic conditions that could compromise maternal health. Women should contact their provider if they have any concerns during their pregnancy.
CDC’s Response
The National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP) works in four key areas or domains: epidemiology and surveillance, environmental approaches, health care system interventions, and community programs linked to clinical services. This comprehensive approach supports healthy choices and behaviors, makes healthier options more available, and helps Americans better manage their health.
CDC works with partners—such as public health agencies, other federal agencies, academia, and community organizations—to improve the health of women before, during, and after pregnancy. With $46 million in FY 2016 funding, CDC’s Division of Reproductive Health supports these efforts by focusing its activities in two of NCCDPHP’s four domains: epidemiology and surveillance and health care system interventions.
Epidemiology and Surveillance
Pregnancy Risk Assessment Monitoring System (PRAMS)
In 1987, PRAMS began collecting state-specific population data on maternal attitudes, experiences, and health before, during, and shortly after delivery. This surveillance system helps to identify women and infants at risk of health problems in order to monitor access to care and services, identify changes in behavior and health status, and measure progress in improving health.
State governments use PRAMS data to plan and review programs and policies that improve health for mothers and infants. For example, Mississippi used responses to supplemental questions on flu vaccination during the 2009-2010 flu season to create briefs for pregnant women and their health care providers to increase awareness and promote vaccination. As a result, the Mississippi Office of Women’s Health and the state’s Immunization Program made policy changes to incorporate PRAMS data into their flu vaccination promotion plan and are also exploring the possibility of allocating funds to give pregnant women free or low-cost flu shots.

Fast Facts
- Each year in the United States, more than 600 women die of pregnancy-related causes, and 65,000 have severe pregnancy complications.
- Chronic conditions, such as high blood pressure, diabetes, heart disease, and obesity may put women at higher risk of pregnancy complications.
- Health care providers and women can work together to prevent and control chronic conditions both before and during pregnancy to improve chances for a healthy outcome.
- CDC provides support to help states track severe pregnancy complications and pregnancy-related deaths. Data from these efforts are used to guide pregnancy care.

Percentage of Women Below, Within, and Above Pregnancy Weight Gain Recommendations, 2013
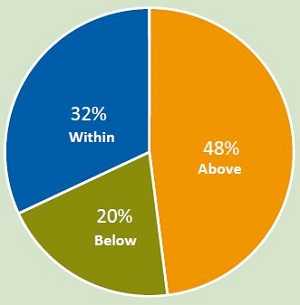
About 1 in 3 women gained the recommended amount of weight during pregnancy. Nearly half gained too much weight.
Source: National Vital Statistics System birth data.
Prevalence of Smoking During Pregnancy, 2013
About 1 in 10 women reported smoking during the last 3 months of pregnancy.
Source: Pregnancy Risk Assessment Monitoring System.
Pregnancy Mortality Surveillance System (PMSS)
In 1986, PMSS started collecting data on women who died while pregnant or within 1 year of the end of pregnancy. Each year, CDC asks 52 reporting areas (50 states, New York City, and the District of Columbia) to send copies of death certificates for these women, along with copies of infant birth certificates or fetal death certificates if they have the ability to link these records. This information is summarized, and medically trained epidemiologists determine if the cause of death is related to the pregnancy.
Causes of death are systematically coded, and PMSS data are used to describe conditions that lead to death, identify risk factors for pregnancy-related deaths, and identify disparities in death rates. Clinicians and public health professionals can use PMSS data to better understand the circumstances surrounding pregnancy-related deaths and take action to prevent them.
“Health outcomes for both mothers and their babies are better today than ever before. We can build on that progress well into the 21st century by continuing to invest in the health and wellness of all women before, during, and after pregnancy.”
Wanda D. Barfield, MD, MPH
Director of CDC’s Division of Reproductive Health

Maternal and Child Health Epidemiology Program
The Maternal and Child Health Epidemiology Program increases states’ epidemiologic capacity by assigning senior CDC maternal and child health (MCH) epidemiologists and fellows to state health departments and other public health agencies. In 2016, 14 senior MCH epidemiologists and 9 MCH fellows from the Council of State and Territorial Epidemiologists were working in 17 public health agencies or institutions. They contribute to programs and policies—such as those intended to increase women’s access to appropriate care during labor and delivery or decrease diabetes, obesity, or high blood pressure among women of reproductive age—that seek to improve the health and well-being of women, infants, children, and families.
As part of their work in 2016, epidemiologists and fellows helped seven states increase their data collection on maternal deaths for their state review committees. They helped an additional three states identify data that can be used to measure the appropriate level of maternity care that hospitals can provide to women at risk during delivery.
As part of their work in 2016, epidemiologists and fellows helped seven states increase their data collection on maternal deaths for their state review committees. They helped an additional three states identify data that can be used to measure the appropriate level of maternity care that hospitals can provide to women at risk during delivery.
Health Care System Interventions
Maternal Mortality Review (MMR) Committees
CDC provides technical assistance and expertise to help states establish MMR committees. These committees help to better identify pregnancy-related deaths, oversee the review of these deaths, recommend actions to help prevent future deaths, and publish review results. CDC works with partners to update national and international recommendations for conducting reviews and for using these data to improve maternal health.
Beyond Our Borders
Building more robust and routine data systems for surveillance of maternal and child health indicators is central to the improvement of data-driven interventions. In addition to its work domestically, CDC provides technical assistance for research, surveillance, and evaluation of interventions in parts of the world with high rates of maternal and neonatal deaths. These efforts are designed to help researchers understand the causes and circumstances that lead to these deaths and to use data for action to prevent deaths.
Future Directions
An important component of CDC’s work in maternal health is improving health outcomes for women who have or may develop chronic diseases during their reproductive years. CDC is strengthening its surveillance for these conditions by:
- Measuring the prevalence of pregnancy-related deaths and complications and their costs in human and financial terms.
- Understanding the causes of pregnancy-related deaths and complications.
- Improving the quality and availability of data needed to monitor chronic conditions that affect maternal health.
- Investigating the effects of preexisting conditions like high blood pressure, diabetes, heart disease, obesity, poor mental health, and substance use on pregnancy outcomes.
- Improving obstetric care and addressing gaps in maternal health care and services.
- Page last reviewed: August 17, 2016
- Page last updated: August 17, 2016
- Content source: