We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Benign paroxysmal positional vertigo
From WikEM
Contents
Background
- Abbreviation: BPPV
- Due to canalolithiasis (migration of otoconia into one of the semicircular canals)
- Mean age is mid-50s; women are twice as likely to be affected as men
- Mean duration is 2 weeks
Clinical Features
- Sudden-onset vertigo and associated nystagmus precipitated by head movements
- Latency period <30s between provocative head position and onset of nystagmus
- Intensity of nystagmus increases to a peak before slowly resolving
- Duration of vertigo and nystagmus ranges from 5–40s
- Repeated head positioning causes vertigo and nystagmus to fatigue and subside
- Nystagmus reverses direction during the head down and head up portions of Dix-Hallpike
- Nausea/vomiting common
- Symptoms worse in the morning (symptoms fatigue as day goes on)
- No associated hearing loss or tinnitus
- MUST distinguish from central vertigo (HINTS Exam, Cerebellar stroke)
Differential Diagnosis
Vertigo
- Vestibular/otologic
- Benign Paroxysmal Positional Vertigo (BPPV)
- Traumatic (following head injury)
- Infection
- Meniere's disease
- Ear foreign body
- Otic barotrauma
- Neurologic
- Cerebellar stroke
- Vertebrobasilar insufficiency
- Lateral Wallenberg syndrome
- Anterior inferior cerebellar artery syndrome
- Neoplastic: cerebellopontine angle tumors
- Basal ganglion diseases
- Vertebral Artery Disssection
- Multiple sclerosis
- Infections: neurosyphilis, tuberculosis
- Epilepsy
- Migraine (basilar)
- Other
- Hematologic: anemia, polycythemia, hyperviscosity syndrome
- Toxic
- Chronic renal failure
- Metabolic
Evaluation
See vertigo for a general approach
Dix-Hallpike Maneuver
- 50-85% Sensitive for BPPV[1]
Procedure
- Patient sits upright
- Patient's head is rotated to one side by 45 degrees. Then quickly lie the patient down
- Maintain the head in 45 degree rotation but also 20 degrees of extension off the end of the table.
- Observe the eyes for 45 seconds for nystagmus. There is often 15 seconds of latency prior to symptoms.
- A positive test for BPPV is evidenced by the rotational nystagmus
- fast phase of the rotatory nystagmus is toward the affected ear, which is the ear closest to the ground
Contraindications[2]
- Concern for Cervical Artery Dissection
- Cerebrovascular disease
- Concern for vertebrobasilar insufficiency, See Stroke syndromes
- Spinal injury
- Cervical spondylosis
Management
Epley Maneuver[3]
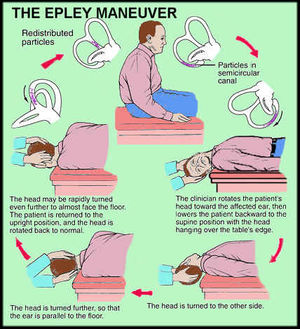
- Epley begins after the last step of the Dix Hallpike
- Patient remains in the position with exacerbated nystagmus for approximately 1–2 minutes.
- Patient's head is then turned 90 degrees to the opposite direction so that the unaffected ear faces the ground
- Maintain the 20 degree neck extension
- Keep the head and neck in a fixed position while the patient rolls onto their opposite shoulder. The patient is now looking downwards at a 45 degree angle.
- Keep the patient in the new position for 1 minute.
- Finally bring the patient up to sitting while holding the head in 45 degree rotation.
- May require multiple attempts, but you can discharge patient home with daily exercises
- Improvement after x1 in 47% of patients, after x2 an additional 16%, and after x3 an additional 21%[4]
Medical management
- Antihistamines
- Diphenhydramine (Benadryl) 25-50mg IM/IV/PO q4hr
- Meclizine(Antivert, Antrizine, Dramamine) 25mg PO QID
- Promethazine(Phenergan, Anergan, Prorex) 12.5-25mg PO/IM/IV q4-6hr
- Anticholinergic
- Scopolamine transdermal patch 0.5mg (behind ear) QID
- Benzodiazepines
Disposition
- Consider referral to ENT for persistent symptoms despite treatment
See Also
External Links
- YouTube: How to do Epley Manuever
- Dix-Hallpike and Epley Maneuvers for BPPV, in Claymation
- Home Treatments of Benign paroxysmal positional vertigo
References
- ↑ Sacco RR et al. Management of Benign Paroxysmal Posi- tional Vertigo: A Randomized Controlled Trial. J Emerg Med. 2014 Apr;46(4):575-81
- ↑ Humphriss, Rachel; Baguley D; Sparks V; Peerman S; Mofat D (2003). "Contraindications to the Dix-Hallpike manoeuvre : a multidisciplinary review". International Journal of Audiology 42 (3): 166–173.
- ↑ Hilton, Malcolm P; Pinder, Darren K (2004). "The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo". In Hilton, Malcolm P. Cochrane Database of Systematic Reviews
- ↑ Hughes D, Shakir A, Goggins S, et al. How many Epley manoeuvres are required to treat benign paroxysmal positional vertigo? J Laryngol Otol. 2015; 129(5):421-424.